After the shock of a prostate cancer diagnosis, the first thing your medical team will talk about is its stage. This might sound like more medical jargon, but it’s actually the most important step in getting a clear picture of what’s happening and what comes next. Think of it as creating a map of the cancer, where it is, how big it is, and if it has started to travel.
When you first hear the words "prostate cancer," it’s completely normal for your mind to race. The diagnosis can feel huge and frightening. Staging is the process that cuts through the uncertainty. It helps translate a scary diagnosis into a manageable set of facts. You could think of it like assessing a fire: is it a small, contained campfire, or has it started to spread to the surrounding woods?
Staging gives your entire healthcare team a shared, precise language to talk about your specific cancer. It’s far more than just a label; it’s a detailed summary that boils down to three core questions:
Getting a handle on these answers puts you back in the driver's seat. It equips you to have better, more productive conversations with your doctors and helps you make decisions that feel right for you and your life.
It's more important than ever for men to understand prostate cancer staging. Why? Because more of us are being diagnosed. Over the last ten years, there’s been a significant jump in diagnoses, thanks to better awareness and more men getting checked. Some national health figures show cases climbing from around 45,000 to over 64,000 over a recent decade, a 42% increase. Even more telling, some data showed diagnoses shot up by an incredible 24% in a single year.
We’ve created this guide to take the mystery out of the staging process. The aim is to turn complex medical terms into simple, understandable ideas, so you have the confidence to face your diagnosis head-on.
Sometimes, the first sign something is wrong is a change in toilet habits. If you're concerned, you might find our article on frequent urination and prostate cancer helpful. But no matter how you arrived here, knowing your stage is the first, most crucial step on your path to treatment and recovery.
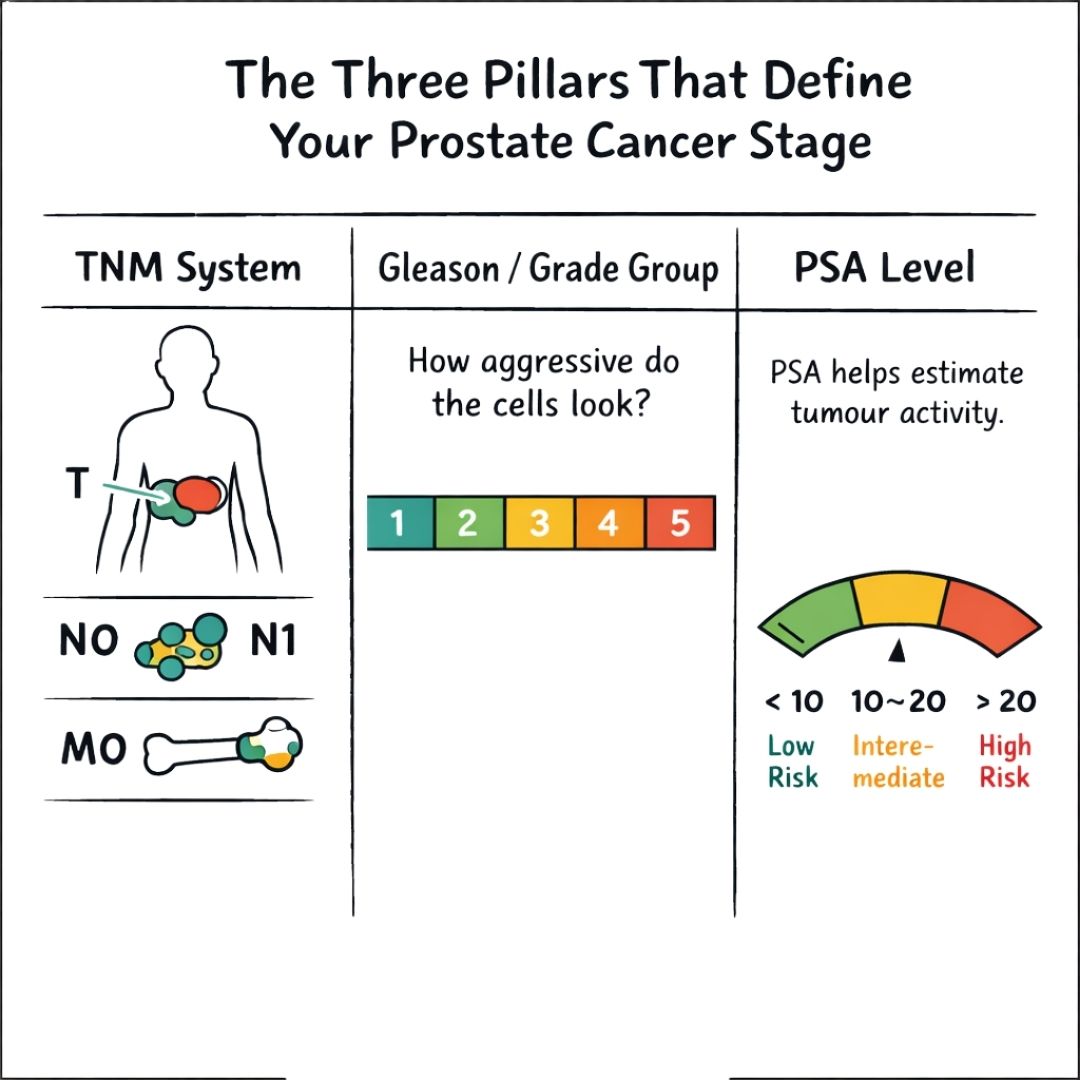
When you’re diagnosed with prostate cancer, your medical team starts piecing together a puzzle. Their goal is to build a complete picture of the cancer, and to do that, they rely on three main pieces of information. Think of them as the three pillars of staging; each one provides a different clue, and only by looking at all three together can they understand the full story.
These key factors are the TNM system, the Gleason score (or Grade Group), and your PSA level. Let's break down what each of these means for you, so you can feel more confident in conversations about your diagnosis and treatment.
The TNM system is a bit like an anatomical map of the cancer. It’s a standardised method used for many cancers, and it focuses on the physical size and location of the tumour. Each letter gives your doctor a specific detail:
T is for Tumour: This tells us about the size and extent of the main tumour within the prostate. A low 'T' number, like T1, means the tumour is small and contained. A higher number, such as T3 or T4, signals that the tumour has grown larger, maybe even breaking through the prostate's outer capsule or into neighbouring tissues.
N is for Nodes: This checks whether the cancer has spread to nearby lymph nodes in the pelvis. Lymph nodes are the small, bean-shaped glands of your immune system that can act as a transport system for cancer cells. An ‘N0’ finding is good news, it means no cancer was found in the nodes. ‘N1’ means it has spread there.
M is for Metastasis: This is the crucial question of whether the cancer has spread (metastasised) to distant parts of the body, like the bones, liver, or lungs. ‘M0’ means the cancer is still confined to the local prostate area, while ‘M1’ confirms it has travelled to other sites.
By combining these T, N, and M values, your doctor gets a clear blueprint of the cancer's physical footprint.
If the TNM system tells us where the cancer is, the Gleason score tells us how aggressive it appears. When a pathologist examines your biopsy tissue under a microscope, they're looking at the cells' behaviour. How different do they look from healthy prostate cells?
The pathologist identifies the two most common cell patterns in the sample and gives each a grade from 3 to 5. These two numbers are added to get the final Gleason score, which will be somewhere between 6 and 10.
A lower Gleason score (like a 6) suggests the cancer cells look more like normal tissue and are likely slow-growing. A higher score (8, 9, or 10) points to a more aggressive, unpredictable cancer that's more likely to grow and spread quickly.
Because the Gleason score can be a bit confusing, especially with a score of 7, it's now often simplified into Grade Groups. This newer system, from 1 to 5, gives a much clearer sense of the cancer's likely behaviour.
Grade Group System
| Grade Group | Gleason Score | Cancer's Likely Behaviour |
|---|---|---|
| 1 | 6 | Low-grade; likely to be slow-growing. |
| 2 | 7 (3+4) | Intermediate-grade; favourable outcome. |
| 3 | 7 (4+3) | Intermediate-grade; unfavourable outcome. |
| 4 | 8 | High-grade; likely to be aggressive. |
| 5 | 9-10 | High-grade; very aggressive. |
This 'report card' on the cancer's personality is a vital piece of the puzzle for predicting risk and deciding how to approach treatment.
The final pillar is your Prostate-Specific Antigen (PSA) level. PSA is a protein made by prostate cells—both healthy and cancerous ones. A simple blood test measures how much of it is in your system, with the result given in nanograms per millilitre (ng/mL).
A high PSA doesn't automatically mean cancer; other conditions like an enlarged prostate can also raise it. But once cancer has been confirmed, your PSA level at diagnosis becomes an important staging marker. It’s like a barometer for tumour activity.
Generally speaking, a higher PSA level can indicate a larger tumour or a more advanced cancer. As a rule of thumb, a PSA level below 10 ng/mL is considered low risk, 10-20 ng/mL is intermediate risk, and anything above 20 ng/mL is considered high risk.
By bringing together your PSA level with the TNM map and the Gleason/Grade Group report, your team can build a comprehensive profile of your prostate cancer.
Once your medical team has gathered all the key pieces of the puzzle, the T, N, and M stages, your Gleason score, and your PSA level, they put it all together to assign an overall stage. While all those individual letters and numbers are quite technical, the final stage grouping is much more practical. It boils all that data down into a clear, big-picture summary of where things stand.
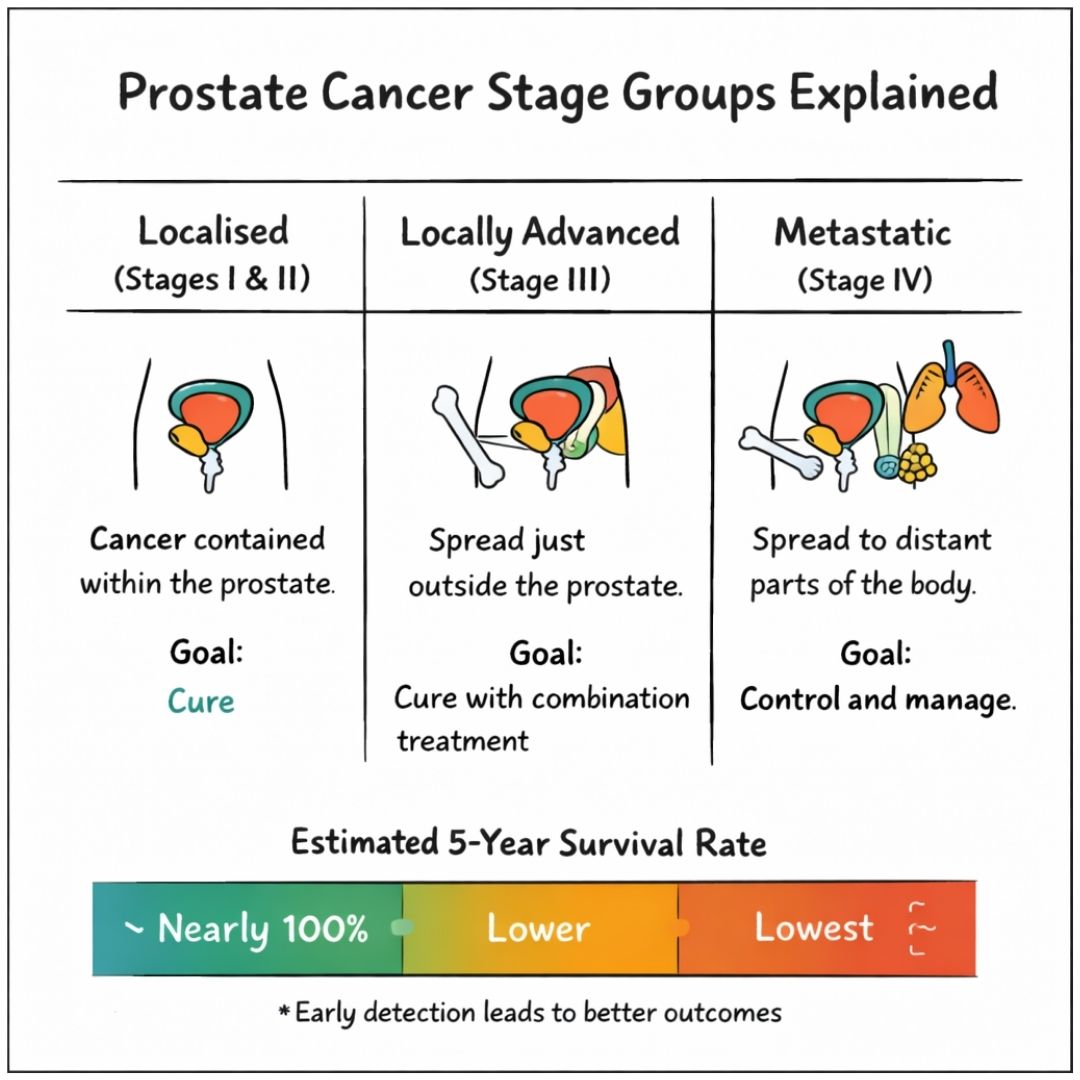
Think of it like this: the TNM, Gleason, and PSA are the specific ingredients, but the stage group is the name of the final dish. It tells everyone what you’re dealing with and points the way forward. Doctors generally talk about three main groups for prostate cancer, and understanding these is key to your treatment conversations.
The main groups are:
Each one paints a picture of how far the cancer has progressed, what it means for your outlook, and what the goals of treatment are likely to be.
This is the earliest stage. Localised prostate cancer means the cancer is found only within the prostate gland itself. It hasn't broken out.
To use an analogy, it's like a small fire burning neatly inside a fireplace. It hasn't spread to the carpet, the walls, or any other part of the house. This is the best-case scenario for a diagnosis.
This stage is often broken down further into risk levels (low, intermediate, or high) based on your Gleason score and PSA. For instance, a man with a low Gleason score of 6, a low PSA, and a small, contained tumour would be considered to have low-risk localised prostate cancer.
What it means for you: The fantastic news is that at this stage, the cancer is considered curable. The primary goal of treatment is to get rid of the cancer completely. This is usually done with surgery (radical prostatectomy) or radiation therapy. For some very low-risk cancers, we might even recommend active surveillance, where we monitor things closely and only step in with treatment if there are signs of change.
Locally advanced prostate cancer describes a situation where the cancer has started to push beyond the prostate's outer boundary (the capsule). It may have grown into the seminal vesicles, which are the small glands next to the prostate that help make semen, or into other tissues right beside it.
The crucial difference here is that the cancer has not yet spread to distant parts of the body, like the lymph nodes or bones. Going back to our fire analogy, the flames have now started to lick the edges of the fireplace and scorch the nearby wall, but the fire is still contained in that one room.
What it means for you: While this is certainly more serious than localised cancer, a cure is often still the goal for Stage III. Because the cancer is no longer neatly contained, treatments usually need to be a bit more intensive. A very common and effective approach is combining radiation therapy with hormone therapy to attack the cancer from different angles.
This is the most advanced stage. Metastatic prostate cancer means the cancer cells have broken away from the prostate and travelled to other parts of the body. The "sparks" from the fire have jumped and started new fires in other rooms of the house.
For prostate cancer, the most common place for it to spread is the bones. However, it can also go to the lymph nodes, liver, or lungs. In the TNM system, this is what the M1 classification signifies.
There's some encouraging news here. Recent data shows that the proportion of men diagnosed with metastatic disease at the outset is falling in some countries, suggesting we are getting better at catching it earlier. That said, significant regional differences persist. In some parts of the UK, for instance, a higher percentage of men are diagnosed at stage four compared to other areas. You can explore the latest data on rising prostate cancer cases and regional trends.
What it means for you: At this stage, the cancer is not considered curable. The focus of treatment pivots from trying to eliminate the cancer to controlling its spread, managing any symptoms it causes, and extending your life while maintaining the best quality of life possible. Treatments are systemic—meaning they work throughout your whole body—and can include hormone therapy, chemotherapy, and newer targeted drug therapies.
To help you see how these stages fit together, this table gives a quick overview of the main groupings.
| Stage Group | Description | Common Treatment Goal |
|---|---|---|
| Localised (I & II) | The cancer is entirely contained within the prostate gland. | Cure. Eliminate the cancer completely with treatments like surgery or radiation, or monitor it with active surveillance. |
| Locally Advanced (III) | The cancer has spread just outside the prostate to nearby tissues, but not to distant parts of the body. | Cure. Use more intensive treatments, often a combination like radiation and hormone therapy, to destroy the cancer. |
| Metastatic (IV) | The cancer has spread (metastasised) to distant parts of the body, such as the bones, lymph nodes, or other organs. | Control. Slow the cancer's growth, manage symptoms, and extend life while preserving quality of life using systemic therapies. |
Seeing it laid out like this can help clarify what each stage means in practical terms and how your doctors will approach planning your care.
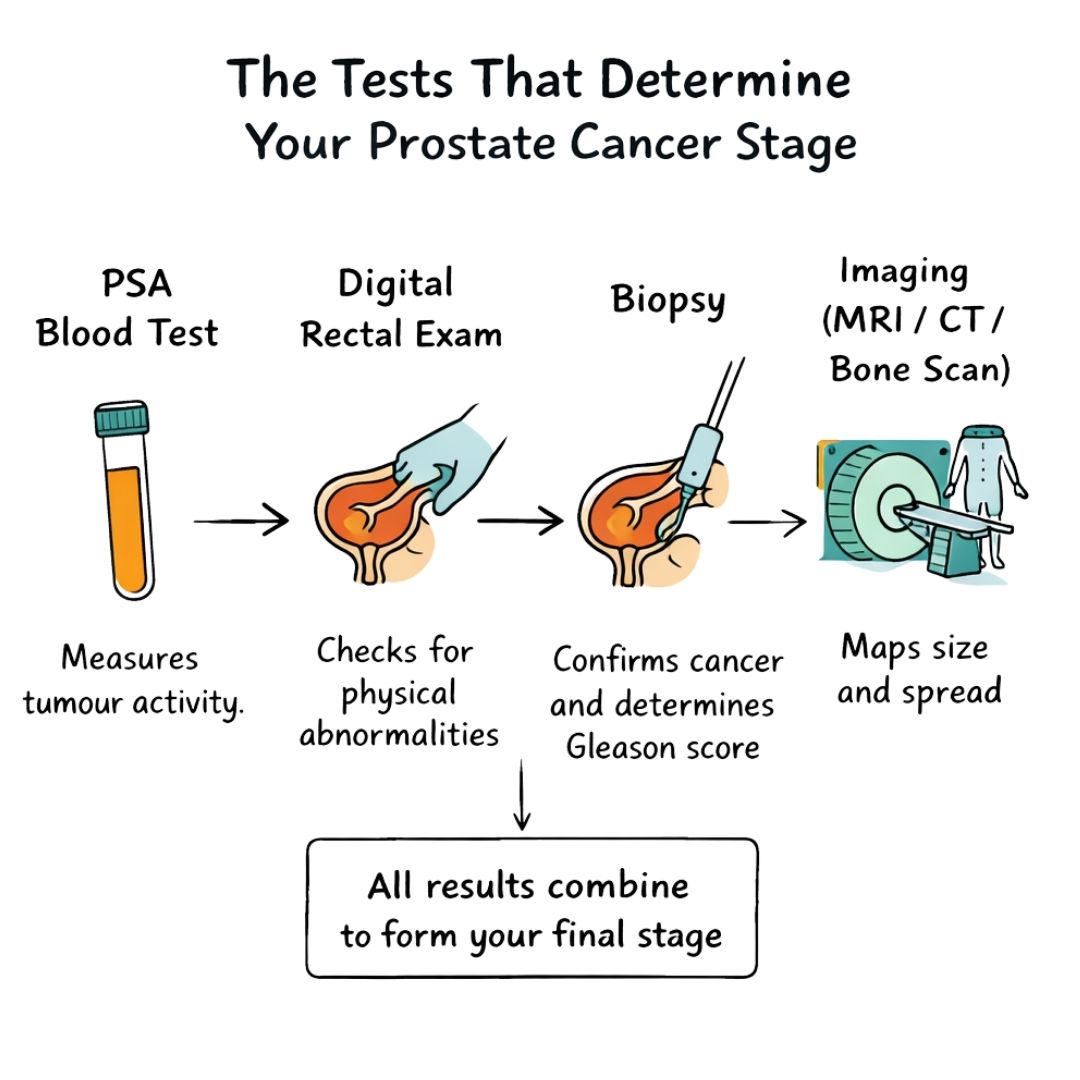
Figuring out the stage of prostate cancer can feel a bit like putting together a complex puzzle. Your medical team will use several different tests, and each one provides a crucial piece of the overall picture. Once you understand what each test is looking for, the process can feel much less daunting and you'll be better equipped to discuss the results with your doctors.
The journey usually starts with a couple of foundational tests. These first steps give your doctor an initial sense of what's happening with your prostate and help them decide if they need to dig a little deeper.
The first test nearly every man has is the Prostate-Specific Antigen (PSA) blood test. PSA is a protein made by your prostate. Now, a high PSA level doesn't automatically mean you have cancer; things like an infection or just an enlarged prostate can also raise it. But it is a very important early warning signal.
To learn more about what your results might mean, you can read our detailed guide on the Prostate-Specific Antigen test.
Next up is often the Digital Rectal Exam (DRE). It's a quick physical check where your doctor feels the prostate gland for any hard areas, lumps, or other unusual signs. Combining the PSA result with the findings from a DRE gives your doctor a much clearer idea of whether a biopsy is the right next step.
If your first tests raise any concerns, a prostate biopsy is the only way to know for sure if cancer is present. This procedure is absolutely vital for staging, as it's the only way to get a tissue sample for a pathologist to analyse under a microscope.
A specialist uses a very thin needle to take several small cores of tissue from different parts of the prostate. Looking at these samples achieves two critical things:
Without a biopsy, you simply can't get a Gleason score or an ISUP Grade Group. This score is a cornerstone of staging because it tells your team about the cancer's "personality"—is it slow-growing and less of a threat, or is it aggressive and likely to spread?
Once a biopsy confirms cancer, your doctor may order imaging tests to see exactly where it is and if it has spread. You can think of these scans as creating a detailed, 3D map of your body. It's important to know that not everyone needs every scan; the decision is based on your specific risk factors, like a high PSA level or a high Gleason score.
The real purpose of imaging is to complete the TNM staging. These scans help your doctor accurately determine the tumour's size (T), whether it has reached the lymph nodes (N), and if it has metastasised to distant parts of the body (M).
Some of the most common imaging tests include:
Each of these tests, from the simple blood draw to the advanced scans, plays a specific and vital role. They are the building blocks that, when put together, define your unique cancer stage and give you and your team the clarity needed to plan the best possible treatment.
Receiving your cancer's stage is a pivotal moment. Think of it as the main map your medical team uses to navigate your treatment journey. But it’s not the only thing they’ll consider. Your age, your general health, and what’s most important to you will all play a crucial part in the conversation.
Deciding on a treatment path is a partnership between you and your doctors. The aim is always to find the right balance—treating the cancer effectively while protecting your quality of life as much as possible. The types of conversations you'll have will look very different depending on whether the cancer is localised, locally advanced, or has spread.
When prostate cancer is localised, it means the tumour is neatly contained within the prostate gland itself. This is the earliest and most common scenario, and thankfully, the outlook is excellent. With the cancer in one specific place, a cure is often the primary goal.
You and your doctor will explore several well-established options:
Choosing between these depends on the specific risk level of your cancer (judged by your Gleason score and PSA), your age, and your own feelings about the potential side effects of each treatment.
Locally advanced means the cancer has started to push beyond the prostate's outer layer, perhaps growing into nearby structures like the seminal vesicles. The good news is that it hasn't spread to distant parts of the body, so a cure is still very much on the table.
Because the cancer is no longer perfectly contained, the treatment plan needs to be a bit more robust.
For Stage III cancer, a single treatment often isn't enough. Combination therapy is the standard of care, designed to attack the cancer from multiple directions and mop up any cells that may have started to escape.
A common and very effective strategy combines radiation therapy with hormone therapy. Hormone therapy works by cutting off the supply of male hormones (androgens) that prostate cancer cells use as fuel. To learn more about this, our guide on hormone therapy for prostate cancer offers a detailed explanation. This one-two punch helps shrink the cancer, making it more susceptible to the radiation.
When prostate cancer becomes metastatic, it has travelled to other parts of the body, most often the bones. At this advanced stage, the cancer is no longer considered curable. The entire focus of treatment shifts from getting rid of the cancer to controlling it.
The goal is to manage the cancer as a chronic illness. Doctors aim to slow its growth, relieve symptoms, and help you live as long and as well as possible. The treatments used are systemic, meaning they travel through your bloodstream to work throughout your whole body. These options include:
The stage at which the cancer is found has a massive impact on the outcome. For men with localised or regional-stage disease, the five-year survival rate is incredibly high, approaching 100% in many countries. However, for men diagnosed after the cancer has spread to distant sites, the survival rates are much lower, with global estimates often around 30-40%.
These figures highlight just how much of a difference early detection makes. While treatments have come a long way, finding and treating prostate cancer before it has a chance to spread is still the most powerful tool we have.
Taking in all the details about prostate cancer staging can feel like a lot to handle at once, and it's completely understandable if you feel overwhelmed. But think of it this way: this knowledge is the first, most important tool you have for taking an active part in your own care. This is a journey you don’t have to walk alone, and taking organised, practical steps can make a world of difference in feeling more in control.
Your first, most powerful action? Get ready for your next appointment. Think about everything you've just learned and jot down every single question that pops into your head, no matter how small or silly it might seem. Coming prepared helps you get the most out of the time with your medical team and find the clarity you need.
A cancer diagnosis isn't just a medical issue; it's a deeply personal one that touches every aspect of your life. This is the time to lean on your family and friends. Don't be afraid to share what you're going through and tell people exactly how they can help, whether that means driving you to an appointment or just being a good listener.
It’s also worth remembering that getting a second opinion is a standard and very sensible step. It can bring peace of mind, confirming your diagnosis and treatment plan are on the right track. Sometimes a different specialist might offer a new perspective or simply reinforce the advice you’ve already been given, which can boost your confidence moving forward.
Open and honest communication is the cornerstone of good cancer care. Be frank with your medical team about your fears, your treatment goals, and your priorities for your quality of life. This ensures your care plan truly reflects what matters most to you.
As you plan for the future, looking into practical matters like cancer life insurance can be a significant step in securing peace of mind for you and your family.
Beyond your inner circle, there’s incredible comfort in connecting with others who truly get what you’re experiencing. You’re not the first person to travel this path, and there's immense strength to be found in shared stories. Thankfully, numerous organisations offer expert information and supportive communities.
Here are a few trusted resources to help you get started:
If you need more specific information on advanced disease, you can find it in our detailed article about metastatic prostate cancer. Ultimately, understanding your stage is the key that unlocks the door to informed decisions, effective treatment, and a strong support system.
When you're trying to get your head around a prostate cancer diagnosis, the details of staging can throw up a lot of new questions. Let's walk through some of the most common ones with clear, straightforward answers to help make sense of it all.
This is a really common point of confusion. Your initial stage, which is figured out when you’re first diagnosed, is set in stone. Think of it as a permanent record of what the cancer looked like at that specific moment.
Now, if the cancer comes back or spreads after you've had treatment, doctors will call this 'recurrent' or 'progressive' disease. They'll keep a close eye on things with regular PSA tests. If they spot any changes, they will re-evaluate the situation to decide on the best next steps for managing it. For some men, this process can bring on symptoms like night sweats, and you can read more about the connection between night sweats and prostate cancer in our dedicated article.
The clinical stage is your doctor’s best initial assessment. It’s based on all the information gathered before any surgery, like the results from your physical exam, biopsy, and imaging scans. It’s essentially the first draft or educated estimate of how far the cancer has spread.
The pathological stage, on the other hand, is the definitive verdict. This can only be determined after a surgeon has removed the entire prostate (in a radical prostatectomy). A pathologist then examines the prostate gland and nearby tissues under a microscope, giving the most precise picture of the tumour's actual size and whether it had started to break out of the prostate. This becomes the final, confirmed stage.
Your clinical stage helps guide the first conversations about treatment, but the pathological stage provides the most accurate information for your long-term outlook. It’s the difference between an estimate and the final measurement.
Not necessarily, and this is a crucial distinction. A high Gleason score (like an 8, 9, or 10) or a high Grade Group (4 or 5) tells you that the cancer cells themselves are aggressive. This means they look very different from normal cells and are more likely to grow and spread quickly.
However, your overall 'stage' also factors in the T, N, and M components – that is, the tumour's size and whether it has spread outside the prostate. It’s entirely possible to have an aggressive cancer that is still completely localised (meaning, not advanced). This is exactly why your medical team looks at all three pieces of the puzzle—Gleason/Grade Group, PSA, and TNM stage, to get the complete picture and map out the right treatment plan for you.
We strongly advise you to talk with a health care professional about specific medical conditions and treatments.
The information on our site is meant to be helpful and educational but is not a substitute for medical advice.
Support lymphatic health during cancer recovery. Learn practical tips and expert advice from Kirsty Wales, the Award-Winning Lymphatic Drainage Therapist
A friendly guide to metastatic prostate cancer. Learn about what it is, how it's diagnosed, current treatments, and how to find meaningful support.
I Was Diagnosed With Prostate Cancer In 2017 At The Age Of 57. I Decided To Write A Book That Shares All Of The Intimate Details Of Prostate Cancer Journey
