The word prognosis can stop a family in its tracks. After a bladder cancer diagnosis, many people hear that word and think it means a final answer about how long someone will live. The reaction is understandable as cancer language often sounds colder and more certain than real life is.
In practice, the prognosis of bladder cancer is better understood as a guide. It helps doctors estimate the outcome of the disease, choose the most suitable treatment, and plan follow-up. It isn’t a fixed sentence written in stone. For many patients, the most useful question isn’t “What is the number?” but “What shapes the outlook, and what can still change it?”
Prognosis means the expected course of a disease. With bladder cancer, it reflects the likely outcome or course of the disease a clinical team predicts from factors such as the stage of the cancer, how the cells look under a microscope, and the health condition of the person.
A simple way to understand it is to think of a weather forecast. A forecast may say rain is likely, but it can’t tell one person exactly where each drop will fall. It helps people prepare: they may take an umbrella, change their route, or postpone a journey. Prognosis works in a similar way as it uses patterns seen in many patients to guide decisions, but it can’t predict one individual life with perfect accuracy.
People often hear prognosis as if it means a countdown. That’s one reason clinic conversations discussing prognosis can feel overwhelming as a patient may be trying to absorb survival statistics, scan results, unfamiliar treatment names, and practical worries all at once.
What doctors usually mean is something more careful. They’re trying to figure out the answers to questions such as:
That’s why prognosis is not just about survival statistics. It’s also about planning treatment choices, estimating possible recovery and quality of life, and discussing the need for long-term surveillance.
Useful takeaway: Prognosis is a planning tool, not a personal verdict.
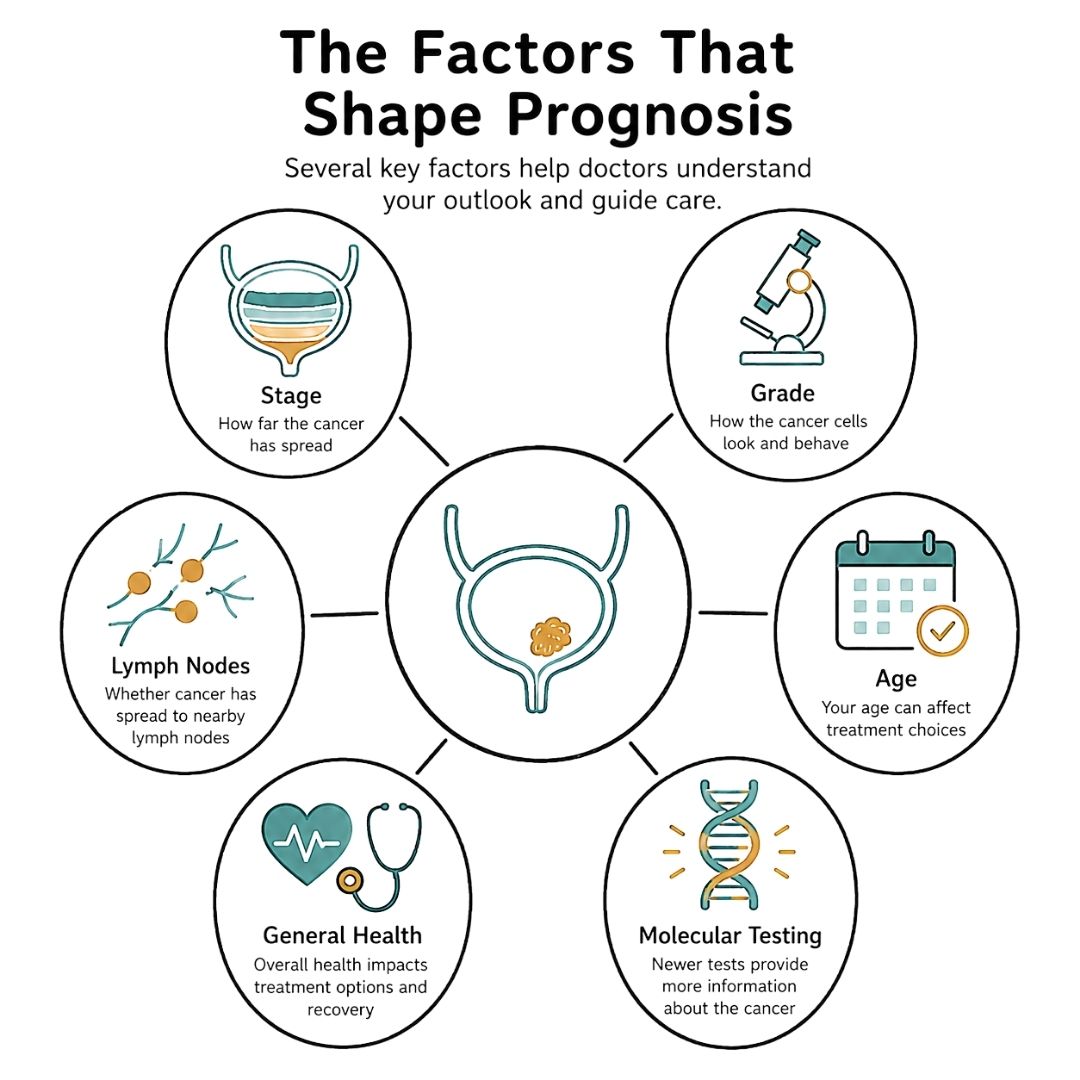
For bladder cancer, a few core factors matter more than anything else.
Stage describes the location and size of the cancer and how far it has spread. The prognosis differs markedly between a tumour confined to the bladder lining, one that has invaded the bladder muscle wall or extended beyond it, and one that has metastasized to distant sites.
Grade describes how normal or abnormal the cancer cells look under a microscope compared to normal cells. Cancer cells with a lower grade grow more slowly and are less likely to spread compared to cancer cells of higher grades, which act more aggressively.
General health matters too. For example, two people can have the same stage of cancer and still have different treatment paths because of different status of kidney function and other medical conditions.
This is why one statistic never tells the whole story. It’s also why many patients benefit from reading clear background on how cancer evidence is interpreted. A plain-language guide to cancer research and biostatistics can make hospital conversations easier to follow.
When understood properly, prognosis can help a family do three important things.
Fear often grows in silence and uncertainty, but clear information replaces helplessness with direction.
Survival statistics can be helpful, but they need careful translation. A phrase such as 5-year survival does not mean a person will only live for five years, but the proportion of people who survive the effect of cancer and are still alive five years after diagnosis in a cohort of patients.
The above distinction matters because these numbers describe populations, not individuals. Survival statistics are derived from a large group of patients, and major factors include age, the stage and type of cancer, and available treatments. Survival statistics offer context, not certainty.
According to bladder cancer survival information from Cancer Research UK, overall 5-year survival is around 50 out of every 100 people, with more than 70% surviving at least 1 year and over 40% reaching 10 years or more.
The main factor of survival statistics is stage. In simple terms, earlier-stage bladder cancer is usually easier to treat than cancer that has grown deeper or spread further. The table below shows the 5-year survival statistics of bladder cancer by stage. The survival statistics are collected from the Surveillance, Epidemiology, and End Results (SEER) Program of the National Cancer Institute of the US and Cancer Research UK.
| Stage | Description | 5-Year Survival |
|---|---|---|
| Stage 0 | Non-muscle-invasive bladder cancer, confined to the inner bladder lining | 98.0% |
| Stage 1 | Non-muscle-invasive bladder-cancer, cancer has invaded the deeper connective tissue but yet the muscle layers of the bladder | 73.0% |
| Stage 2 | Muscle-invasive bladder cancer, cancer has penetrated the muscle layers | Around 50% |
| Stage 3 | Muscle-invasive bladder cancer that has spread to nearby tissues, reproductive organs or lymph nodes | 41.8% |
| Stage 4 | Metastatic bladder cancer, cancer cells spread via the lymphatic system and blood, forming tumors in other parts of the body; a type of muscle-invasive bladder cancer | 9.6% |
This stage pattern helps explain why symptoms such as visible blood in the urine should never be brushed aside. When bladder cancer is found early, the chances of controlling it are much better.
A newly diagnosed patient may look at a table like this and feel either reassured or terrified. Both reactions are understandable, but both can be misleading if the numbers are taken too precisely.
These figures do not say what will happen to one particular person. They don’t include every detail that matters, such as tumour grade, response to treatment, kidney function, or whether the cancer comes back after initial treatment. They also don’t capture how treatment options have changed over time.
Survival statistics are most useful when they answer “What is typical for a group like this?”, not “What will happen to this individual?”
Rather than treating survival figures as a verdict, patients and families can use them to guide more practical questions:
For many readers, this wider context helps when reviewing educational material on current cancer research developments. Good information should reduce confusion, not increase it.
The main message in the survival statistics is clear. The prognosis of bladder cancer varies widely by stage. That’s why early diagnosis, accurate staging, and prompt treatment matter so much.
Two people can receive the same diagnosis and still be given different advice about outlook, treatment, and follow-up. This is because, in practice, your team is building a fuller picture, piece by piece, rather than handing down one fixed answer on day one.
Stage is often the first thing clinicians discuss because it strongly affects prognosis. A cancer limited to the inner lining is managed differently from one that has grown into the bladder muscle or spread beyond the bladder.
This is why terms such as Ta, Tis, T1, or muscle-invasive matter. They describe how deep the cancer has gone and whether it appears to be local or has started to involve nearby tissues or more distant areas.
If those labels sound technical, it may help to translate them into two practical questions. First, how deep is the tumour? Second, has it stayed in one place? Answers to those questions shape both the outlook and the treatment choices offered.
Grade is different from stage. Stage describes location and spread, while grade gives clues about how normal or abnormal the cancer cells look under the microscope compared to normal cells, and how aggressively they may behave.
Some bladder cancers are low-grade (or well-differentiated), which usually means the cancer cells look very similar to normal cells and are growing slowly, and thus being less likely to invade quickly. Cancer cells of intermediate grade (or moderately differentiated) look more abnormal and less similar to normal cells. High-grade cancer cells, which are also described as poorly differentiated or undifferentiated, look most abnormal. They are more likely to grow and spread quickly, and thus, more aggressive treatment and surveillance may be needed.
That is why “early-stage” bladder cancer still needs serious attention. A tumour may be small or localized, but if the cells are high-grade, the risk picture changes.
Aging is associated with an increase in the risk of bladder cancer. Cancer Research UK notes that bladder cancer incidence rises with age, as shown in its bladder cancer incidence statistics by age.
What often matters just as much is general health. Doctors look at kidney function, heart health, mobility, frailty, and how independent someone is day to day. These factors determine which treatments are realistic and safe.
For instance, a fit older adult may cope well with major treatment, while a younger person with serious pre-existing medical conditions may need a different plan.
Therefore, it can be seen that prognosis is best understood as a guide that changes with new information. It is linked to the cancer itself, but also to what treatment the body can tolerate.
Another part of the picture is whether cancer cells have reached nearby lymph nodes. These are small, bean-shaped structures that help filter lymph fluid, and one of the places bladder cancer cells can travel first.
Lymph node invasion is observed in Stage 3 or 4, which are classified as muscle-invasive bladder cancer. Standard treatment for muscle-invasive bladder cancer involves chemotherapy followed by radical cystectomy (RC) with pelvic lymph node dissection (PLND). And, urinary diversion will be done to allow urine excretion from the body. Specifically, for Stage 3, a combination of chemotherapy and radiation therapy may also be used. For Stage 4, treatment strategies depend on whether the cancer is locally advanced or metastatic. Patients trying to make sense of surgical reports may find a plain-language guide to lymph node removal helpful during discussions about cystectomy or pathology results.
Cancer care is becoming more individualized. Pathology findings, scan results, and in some settings newer molecular or blood-based tests can help clinicians estimate risk more precisely.
While that does not remove uncertainty, it does mean prognosis is less like a fixed sentence and more like a working map. As test results come in and treatment begins, the map becomes clearer.
For patients and families, such shift matters. It means better questions can lead to better decisions, and your outlook may be refined as the team learns more about both the cancer and how you respond to treatment.
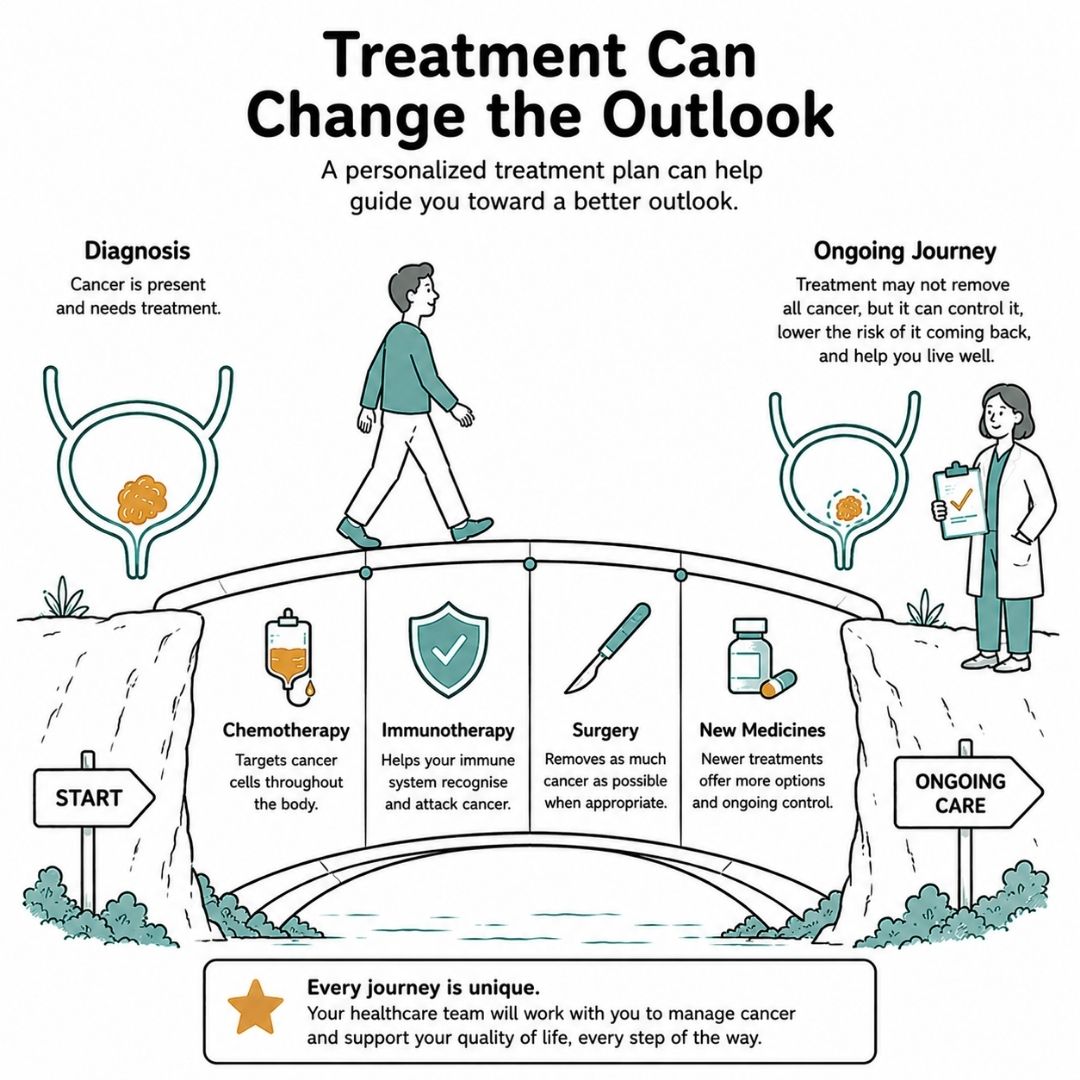
A family often hears the word prognosis and pictures a fixed end point. However, please bear in mind that the survival statistics are based on a large cohort of patients that received different types of treatments and responded differently. The prognosis does not define exactly how your cancer will respond to treatment. Therefore, treatment is one of the main reasons prognosis should be seen as a working guide rather than a sentence set in stone.
Different types of treatment can alter the prognosis in different ways. Some treatment options help to improve the outlook by stopping the spread of cancer, which suit those aiming to keep the cancer under control, slow it down, shrink it, or relieve symptoms. Some treatments aim at helping a person live longer or better with cancer, while others support the elimination of all visible cancer. Each goal can improve outlook in a real and measurable way.
In non-muscle-invasive bladder cancer (Stage 0 and Stage 1), the first step is often a procedure to remove the tumour from the bladder lining, called transurethral resection (TUR). However, due to the high recurrence rate of Stage 0 and Stage 1 bladder cancer after TUR, most patients are advised to have medicine put directly into the bladder to prevent remission. Options include intravesical chemotherapy and intravesical Bacillus Calmette-Guerin (BCG) therapy, a type of immunotherapy.
When it comes to high-risk non-muscle-invasive bladder cancer, BCG therapy is well-established and the standard of care which can reduce the risk of progression. It activates the immune cells in the bladder to attack bladder cancer cells. Maintenance therapy for up to 3 years with BCG may be advised after TUR.
The difference between recurrence and progression is important. While recurrence of cancer in the bladder lining may still be managed locally, cancer that progresses into the muscle layer is a different problem and often needs more intensive treatment.
Patients and families often find making decisions less intimidating after reading a plain-language guide to what immunotherapy is, especially when newer systemic treatments become part of the conversation.
Once cancer has reached the muscle layer, treatment required usually becomes stronger and more time-sensitive. Surgery to remove the bladder, radical cystectomy (RC), as noted earlier, is a standard approach. Depending on tolerance to chemotherapy, patients are offered neoadjuvant chemotherapy before RC, which has been shown to improve prognosis than surgery alone.
The rationale behind RC with neoadjuvant chemotherapy for muscle-invasive bladder cancer is easy to grasp. While removing the bladder deals with the visible tumour, chemotherapy targets the occult micrometastasis upon diagnosis or cystectomy.
Your medical team will weigh the potential benefits of neoadjuvant chemotherapy against fitness, kidney function, hearing, nerve health, and other medical factors, because the best plan has to be both effective and safe for you.
For metastatic bladder cancer, treatment is no longer limited to one path.
Chemotherapy still has an important role, but immunotherapy and other newer options have given some patients more time and, in some cases, longer periods of control.
Response is not identical for everyone. Uncertainty can feel frustrating, but it is also why prognosis keeps being updated during treatment. Scan results, symptom changes, side effects, and how well the cancer responds all help the team refine the picture.
There is ongoing development of newer tests that may help doctors evaluate risk more precisely after treatment. These tools are still part of a developing area of care, but the wider point is reassuring. Prognosis can become clearer over time because treatment itself provides new information.
Many patients feel a little steadier once they see prognosis and treatment as connected. A survival statistic describing what happened across a group cannot fully capture how one individual may respond to surgery, bladder treatments, chemotherapy, or newer medicines.
A more useful question is often: “What parts of my outlook can treatment still improve?” This question gives patients a more active role as it helps families focus on timing, options, and trade-offs instead of feeling trapped by a number.
You finish treatment, go home, and then a new kind of stress appears. The next cystoscopy is marked on the calendar. A scan date is coming up. Someone in the family asks: “Does this mean the cancer might come back?” That question sits heavily with many people, and it deserves a clear answer.
Recurrence risk is part of bladder cancer care because this disease can behave in a stop-start way, especially when it begins in the bladder lining. Prognosis is still useful here, but it works more like a weather forecast than a final verdict. It helps your team estimate what is more or less likely, and adjust the plan as new information comes in.
Two terms often cause confusion. Recurrence means the cancer returns after treatment. Progression means the cancer has become more advanced, such as growing deeper into the bladder wall or spreading further. A cancer can recur without progressing.
Follow-up is a planned way of checking for change early. In non-muscle-invasive bladder cancer, that often means cystoscopy at set intervals because the inside lining of the bladder can develop new abnormal areas over time. Finding a small change early can give your team more choices and may allow simpler treatment than if it were left to grow.
For many people, cystoscopy becomes the backbone of long-term monitoring. It can feel intrusive and emotionally draining. Even so, it helps in the same way a smoke alarm helps. You hope it stays quiet, but you still want it there.
As for muscle-invasive bladder cancer, a follow-up plan may also include scans, imaging, urine tests, blood tests, and review of any symptoms that are new or getting worse. Blood tests are not a simple stand-alone way to confirm or rule out bladder cancer, but they can help to add in useful pieces of information. If you want a plain-language overview, this guide explains whether cancer can be checked by a blood test.
If bladder cancer is muscle-invasive, locally advanced, or has spread, follow-up has a slightly different purpose. Your team is not only watching for recurrence, but also checking how well treatment is controlling the cancer, how your body is coping, and whether the plan still matches your goals.
That is why appointments may include scans, laboratory tests, symptom review, and discussions about energy levels, pain, urinary changes, or side effects. These visits are active care because they help the team decide whether to continue the current treatment, adjust it, or consider another option. Such ongoing review can also make prognosis more accurate over time.
The stretch between appointments can be hard. Some people feel calm until the week before a scan. Others notice every ache, every trip to the toilet, every change in urine, and wonder if it means the cancer is back. These are all common responses.
A practical plan helps. Ask for a written schedule. Meanwhile, keep a note of symptoms worth reporting urgently, such as visible blood in the urine, worsening pain, fever, difficulty passing urine, or unexplained weight loss. Also, ask which symptoms are expected after treatment such that normal recovery does not create extra fear.
Families often feel steadier when they know who to call, how quickly results usually come back, and what the team is watching for at each visit.
Long-term follow-up can feel repetitive, but it is essential. It provides earlier warning if a problem appears, and more chances to act while choices are still open. Follow-up plan is one of the important tools that helps shape the prognosis over time.
Good questions can change the quality of a cancer appointment by helping patients move from hearing information to understanding it. They also reduce the chance that important details get lost in the stress of the moment.
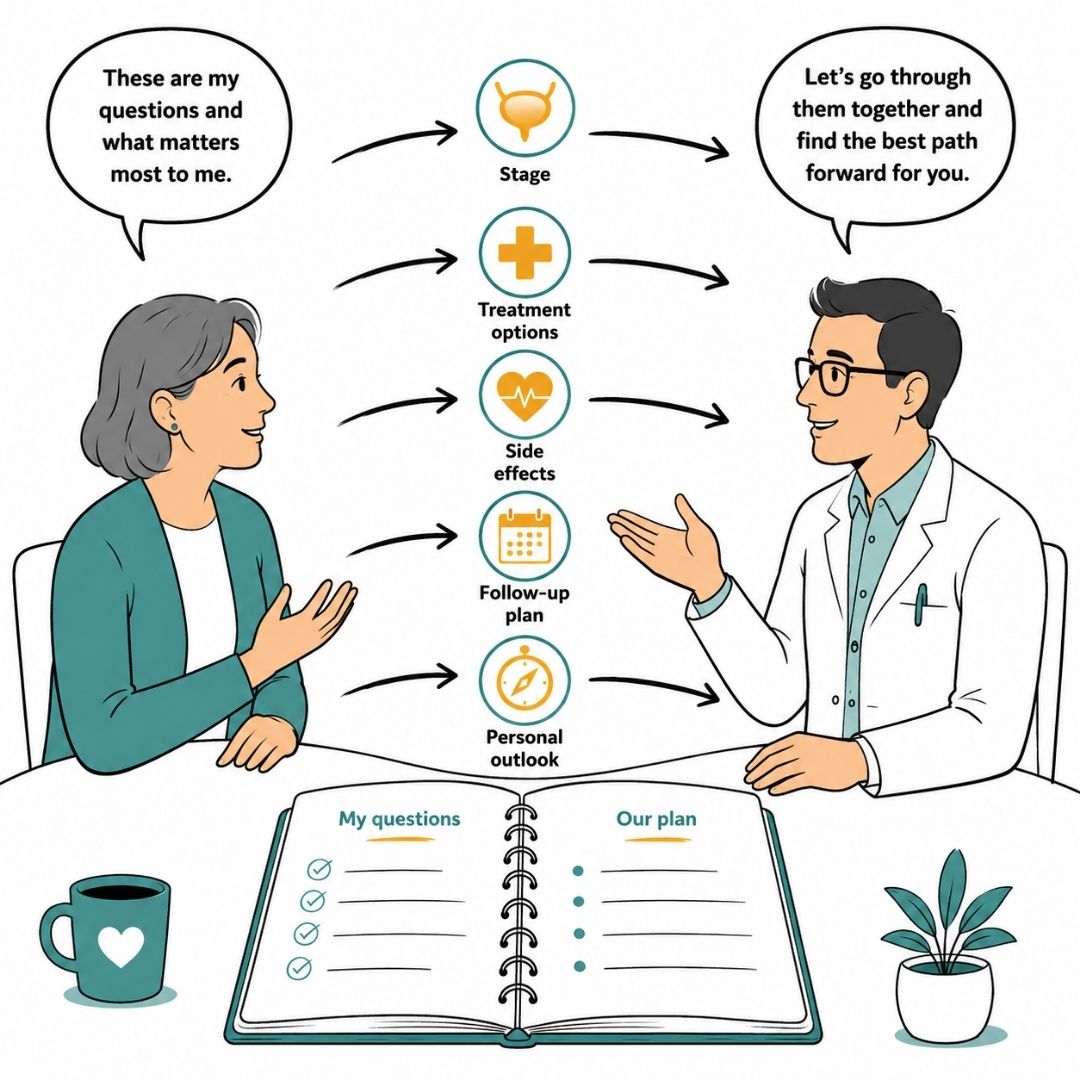
These questions help pin down the basic information about diagnosis:
What is the exact stage of bladder cancer?
This gives the most important starting point for understanding outlook and treatment.
What is the grade of the tumour?
Grade helps explain how active or aggressive the cancer cells appear.
Is it non-muscle-invasive or muscle-invasive?
The difference often changes the treatment plan significantly.
Have any lymph nodes or other areas shown signs of spread?
This can affect both prognosis and the treatment options available.
Some appointments move quickly into treatment names without enough context. These questions bring the conversation back to purpose.
What is the goal of this treatment?
The answer may be cure, control, shrinking the cancer, reducing symptoms, or lowering the risk of recurrence.
Why is this treatment being recommended over other options?
This helps patients understand the reasoning, not just the recommendation.
How might this treatment affect day-to-day life?
Families often need practical information about fatigue, mobility, bladder function, work, and caregiving.
What signs will show whether the treatment is working?
This can include scans, cystoscopy findings, pathology results, or symptom changes.
Taking a written list into clinic often leads to calmer, more focused conversations.
Many people want honest information but don’t know how to ask for it. These prompts can help:
It’s also wise to ask who to contact between appointments if bleeding, pain, difficulty urinating, or treatment side effects become concerning.
A few simple habits can make a major difference:
The prognosis of bladder cancer is not a number that defines one's life. It is a constantly changing clinical picture shaped by stage, tumour behaviour, overall health, treatment response, and careful follow-up.
Patients and families often cope better when they focus on the next useful step. Understand the diagnosis, ask direct questions, follow the treatment plan as closely as possible, keep follow-up appointments, and accept support.
Emotional health needs care too. For readers trying to steady themselves through diagnosis, treatment, or survivorship, this guide on how to maintain mental health during life transitions may be a helpful companion.
We strongly advise you to talk with a health care professional about specific medical conditions and treatments.
The information on our site is meant to be helpful and educational but is not a substitute for medical advice.
It’s a common misconception that Plastic Surgeons only perform cosmetic procedures. Plastic surgery is actually an incredibly broad speciality, covering a wide range of conditions.
Discover Why Post-Surgery Bras Are Crucial After A Mastectomy, Offering Support, Reducing Swelling, And Aiding Recovery. Find The Right Fit For Comfort And Healing.
In This Article, We Focus On The Guidelines And The Type Of Exercise That You Can Do After Mastectomy Or Breast Reconstruction And Other Breast Surgeries.
