
Subtotal: £80.00

Subtotal: £80.00
Subtotal: £80.00
Plastic surgery is actually an incredibly broad specialty, covering a wide range of conditions. Treating cancer patients is a key part of our daily workload, in particular patients with skin cancer or breast cancer.
Skin cancer varies in severity and not all patients who receive this diagnosis need to see a plastic surgeon. For those that do, they will generally have the cancer excised and the resulting skin defect reconstructed. Reconstruction ranges from simply stitching the edges together to transplanting tissue from one part of the body to another.
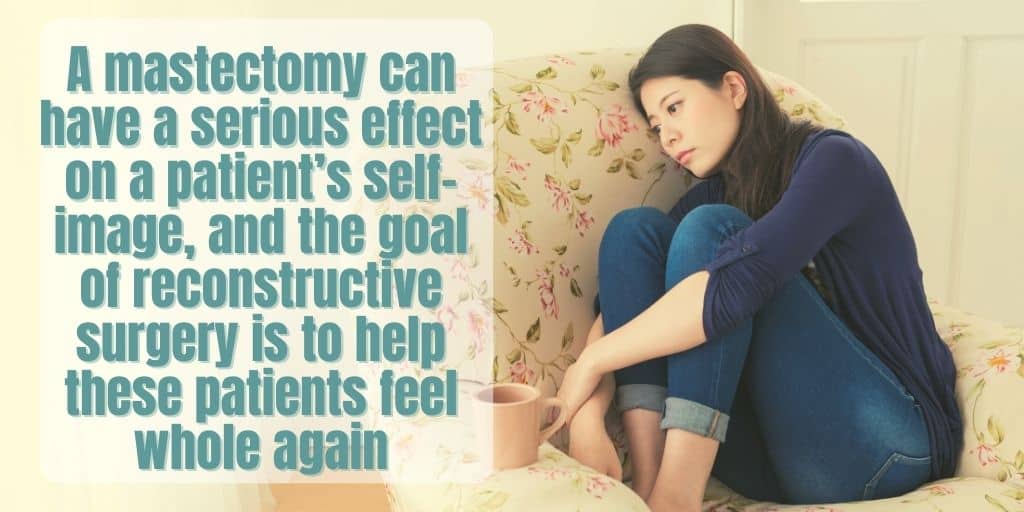
In breast cancer patients, we are generally involved in the reconstruction, which occurs following cancer excision. This a key part of the breast cancer treatment journey and plays a big part in helping patients deal with the psychological aspects of breast cancer. A mastectomy can have a serious effect on a patient’s self-image, and the goal of reconstructive surgery is to help these patients feel whole again.
This is our opportunity to check on the plastic surgery patients who are currently admitted to the hospital. This is most commonly the patients who have had the most complicated types of breast reconstruction and require a few days to recover before they can be discharged. Once we’ve assessed them, we can give the day’s plan of action for each patient to the nursing staff looking after them on the ward. The ward round also allows us to pick up on any problems that the patient is having and deal with them early. Early diagnosis of a surgical complication is key to getting a good outcome, making this a vital part of our day.
In the outpatient clinic, we will often see between 10-30 patients in a morning session. These will be a variety of new referrals and follow-up patients. We tend to spend the most time with our new referrals as there is often a lot to discuss. Particularly in those with skin cancer, we are often involved in breaking the bad news of the cancer diagnosis to the patient and it’s important that these consultations are not rushed.

Where possible, we try to ensure that a nurse specialist is present during the consultation with any patient who has a high-risk skin cancer such as a melanoma. Patients receiving a cancer diagnosis will often have complex emotional issues they need to work through, and our specialist nurses are highly trained to help manage these. They are often less time pressured than us and so are free to give more time to the patient where needed.
With our breast cancer patients, the most time is spent consulting patients at the beginning of their reconstructive journey. There are usually a number of different options available to them and it’s important for them to be fully aware of the pros and cons of each. For example, many patients have the option of either an implant-based reconstruction or transplantation of tissue from another area of their body to recreate the breast. This is a big decision for the patient, as the two operations are very different in terms of surgical complexity and long-term outcomes.
On days where there’s clinic in the morning, we often have half a day of operating in the afternoon. Otherwise, we usually operate for the whole day. Before the list starts, we first have to see and consent the patients for the procedure they’re having. Most of the patients will have had everything explained to them in clinic, but since there’s a lot to take in, we try and summarise the operation again and discuss the risks/benefits. This ensures that the patient is fully on board with what is going to happen and is aware of both the risks and benefits of the procedure.
After consenting the patients, we go and brief the theatre team. This is an important part of the day as it ensures everyone involved in the case knows what the plan is and what their role is. When the team is ready, the first patient is brought round to the operating theatre and the list begins.
For the bigger cases that require a general anaesthetic, there is usually a bit of down-time at this point while the patient is being put to sleep. We often use this to grab some lunch and a quick coffee. When there are lots of patients to see it can be difficult to find time to unwind, so we try and make the most of the breaks we get!
When the patient is asleep, they are transferred to the operating table and prepared for surgery. Their skin is cleaned and sterile drapes are placed around the operating field. There are usually two surgeons who ‘get scrubbed,’ which is the term we use for washing our hands thoroughly and putting on a sterile gown and gloves.

After this, the operation begins. There are usually two surgeons (a lead and an assistant) for each operation, although this can vary depending on the complexity of the procedure. Whilst they are focusing on operating, the anaesthetist will be constantly monitoring the patient to check they are ok throughout the procedure.
When we’ve finished operating and the wound is dressed, the anaesthetist slowly wakes up the patient, and they are transferred to the recovery room where a specialist nurse looks after them until they are fully awake. While this is happening, we try and get the paperwork done for the operation and if possible, grab another cup of coffee!
Finally, once the list is finished, we do another quick ward round of all the patients who have been operated on that day. By this stage, most of the patients are fully alert and anxious to hear how everything went. Following this, provided there are no issues on the ward, we’re free to go home and get some rest before starting it all again the next day!