The call may have ended, the message may still be sitting in your inbox, or you may be waiting for the next scan while your mind races ahead. For many people, the hardest part of a kidney cancer diagnosis is the gap between hearing the words and understanding what they mean for your life.
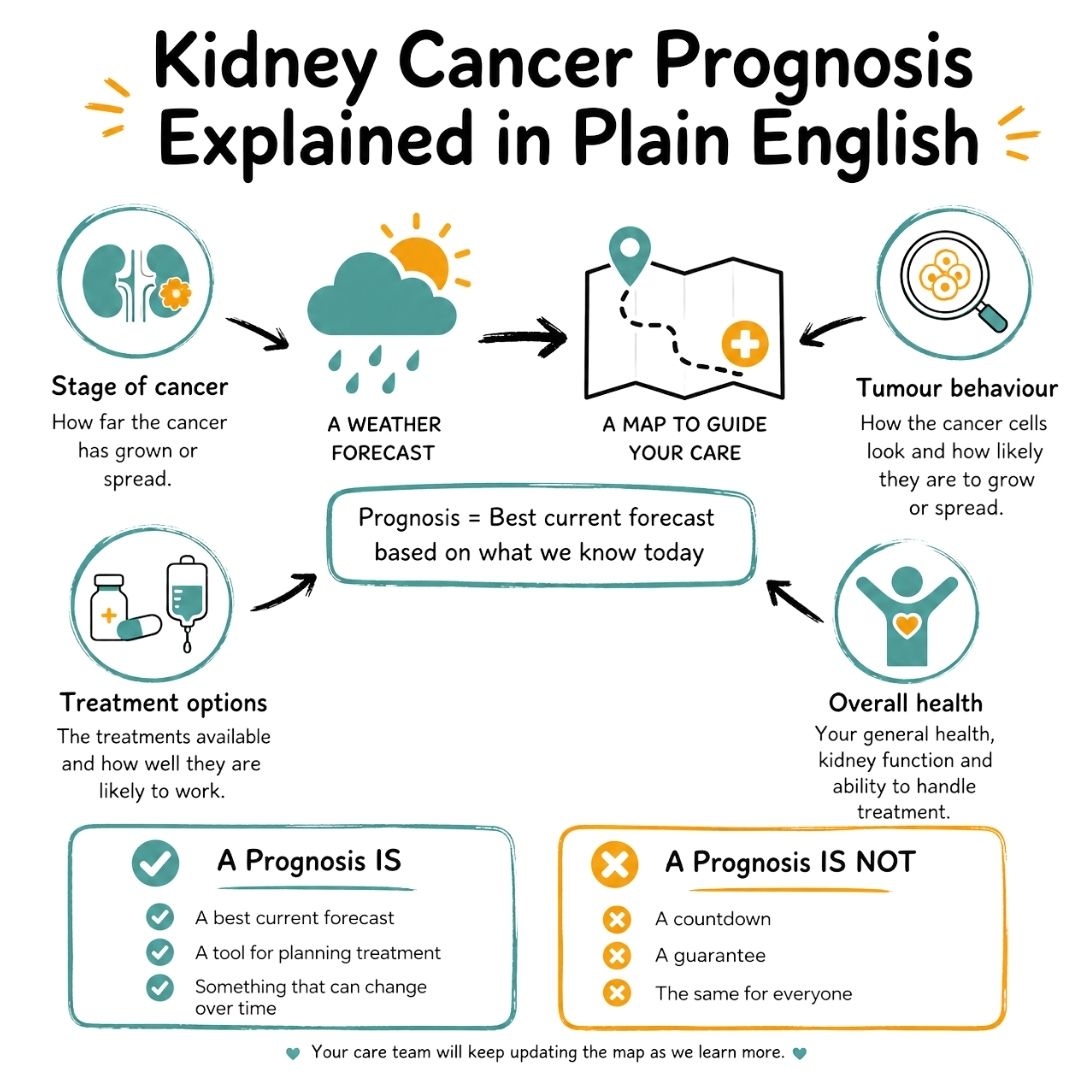
One of the first terms you’ll hear is prognosis. That word can feel heavy. It often sounds like a verdict, when in reality it’s closer to a map. It helps your clinical team judge how the cancer is behaving, what treatments are most likely to help, and what sort of follow-up you may need.
That doesn’t make it easy. It does make it more manageable.
This guide is written to translate kidney cancer prognosis into plain English. If you’re a patient, caregiver, friend, or family member, the aim is to help you move from vague fear to clearer questions, steadier expectations, and more useful conversations in clinic.
A kidney cancer diagnosis often arrives in the middle of ordinary life. You may have gone for a scan for something else. You may have had blood in your urine, pain in your side, or no symptoms at all. Then suddenly you’re learning new terms, meeting unfamiliar specialists, and trying to remember what was said after the word “cancer”.
That fog is normal.
Prognosis is one of the words that can add to the confusion. Many people hear it and think it means a fixed timeline. It doesn’t. It’s your team’s best informed estimate, based on the cancer’s stage, the tumour’s features, your general health, and how kidney cancers like yours tend to respond to treatment.
A prognosis is not a promise and it’s not a countdown. It’s a clinical tool that helps guide decisions.
If your head goes blank in appointments, write questions down beforehand and bring someone with you if you can. A simple prompt list can make a big difference. This guide to questions to ask your oncologist can help you organise what you want to understand before your next visit.
When doctors talk about kidney cancer prognosis, they’re talking about likelihoods, not certainties. The easiest way to think about it is a weather forecast. If the forecast says there’s a high chance of rain, that helps you decide whether to carry an umbrella. It doesn’t tell you exactly what will happen on your street at 3 pm.
Cancer prognosis works in a similar way. Doctors look at information from many patients treated over time. They combine that with what they know about your own cancer. Then they build a picture of what may lie ahead.
A kidney cancer prognosis usually reflects several questions your team is trying to answer:
How localised is the cancer
Is it confined to the kidney, or has it spread beyond it?
How aggressive does it appear
Some tumours behave more slowly, while others are more likely to grow or spread.
What treatments are possible
Surgery, ablation, targeted therapy, and immunotherapy can all affect outlook.
How fit is the person overall
Two people with the same stage of cancer may not have the same treatment options or recovery path.
This is why no doctor can give a perfect personal prediction. Statistics describe groups. Your life is not a group average.
A prognosis doesn’t tell you exactly how long you will live. It doesn’t know how your body will respond to treatment. It doesn’t account for every detail of your daily health, support system, resilience, or future treatment advances.
That uncertainty can feel uncomfortable, but it matters to understand it properly. Many people hear one number and assume it applies directly to them. That’s rarely how oncology works.
Practical rule: When you hear a survival statistic, ask, “What does this mean for someone with my stage, tumour type, and overall health?”
That question shifts the conversation from abstract numbers to your specific situation.
Even though it isn’t exact, prognosis is still useful. It helps doctors choose the right intensity of treatment, estimate the benefit of surgery or drug treatment, and plan surveillance after treatment ends. It also helps patients make practical decisions, from work planning to family conversations.
If you like to understand how medical evidence and patient data are interpreted, this plain-language guide to cancer research and biostatistics can make clinic discussions feel less mysterious.
Try mentally replacing “prognosis” with “best current forecast”. That small shift can reduce some of the fear attached to the word.
The forecast can improve. It can also become clearer over time. After surgery, after scan results, and after seeing how treatment is working, your team often refines what they tell you. In that sense, prognosis is not one conversation. It’s an evolving one.
When people ask about kidney cancer prognosis, they’re often really asking one question: what are the chances of doing well? The most common way doctors discuss that is by talking about stage.
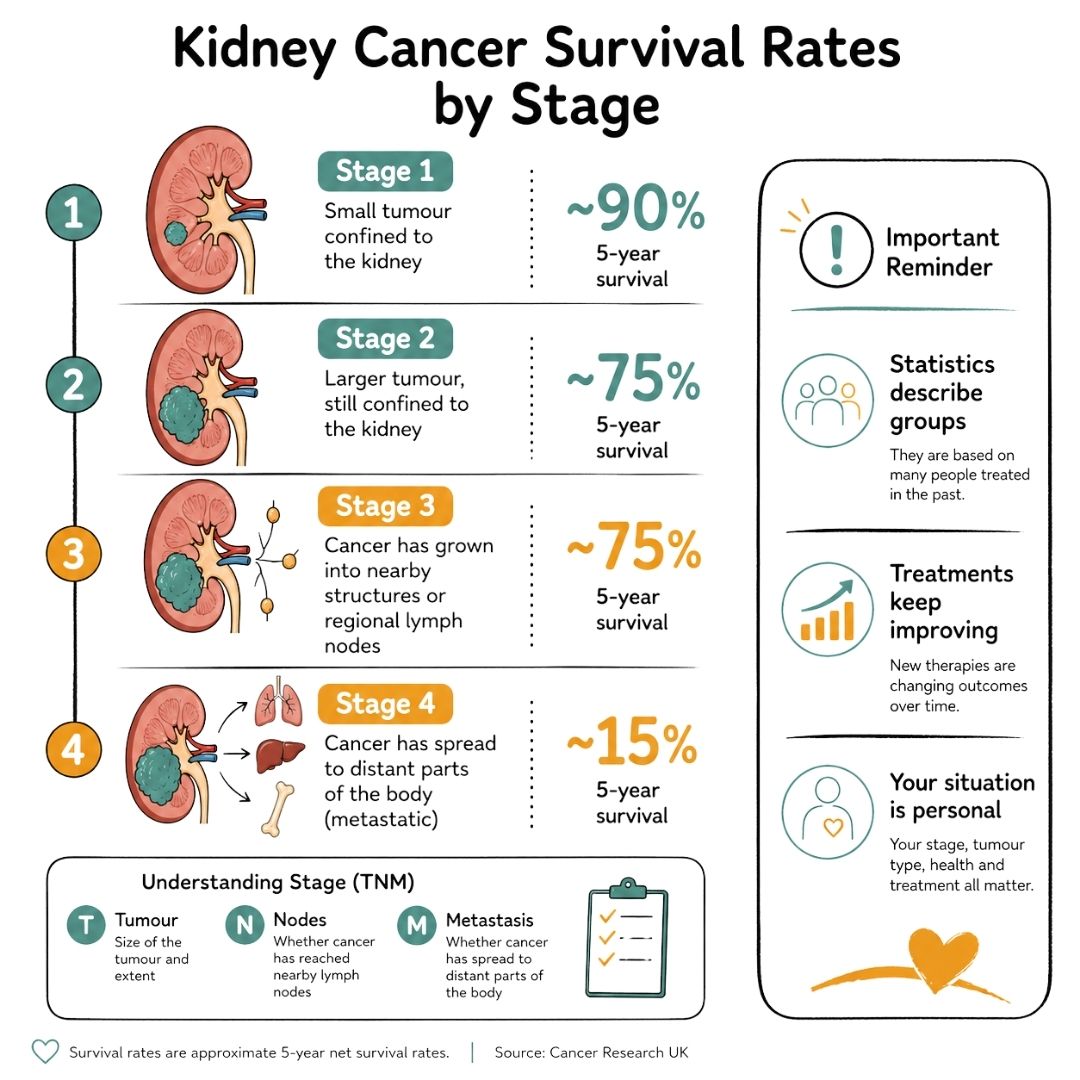
Staging describes where the cancer is and how far it has spread. You may hear the term TNM, which stands for tumour, nodes, and metastasis. In plain language, that means:
Those details are then grouped into stages.
According to Cancer Research UK survival information for kidney cancer, prognosis is strongly linked to stage at diagnosis. The same source also notes that surviving the first year after diagnosis raises the overall chance of surviving five years to over 80%, which is an example of how outlook can change over time.
| Stage | Simplified Description | Approximate 5-Year Survival Rate |
|---|---|---|
| Stage 1 | Small tumour confined to the kidney | Almost 90% |
| Stage 2 | Larger tumour, still confined to the kidney | Around 75% |
| Stage 3 | Cancer has grown into nearby structures or regional lymph nodes | Around 75% |
| Stage 4 | Cancer has spread to distant parts of the body | Around 15% |
These figures are helpful, but they can also be misleading if they’re taken too directly.
They do not mean that every person with stage 2 kidney cancer has the same outcome. They don’t tell you whether your tumour is slow-growing or more aggressive. They don’t tell you whether surgery has removed all visible cancer, or whether your tumour type is likely to respond well to a newer treatment.
They also come from people treated in the past. That matters because treatment keeps changing.
Survival rates are rear-view mirror data. Your treatment plan is made in the present.
Stage matters because it usually tells doctors what can still be removed or controlled locally, and what may need whole-body treatment. If the cancer is confined to the kidney, surgery or ablation may be aimed at cure. If it has spread, treatment often focuses on controlling disease, slowing progression, relieving symptoms, and extending good-quality life.
That distinction can sound frightening, but it’s also practical. It helps patients understand why one person is offered partial nephrectomy, while another is discussing immunotherapy combinations or targeted treatment.
If you know your stage, try asking these in clinic:
What exactly makes this my stage
Ask whether the stage is based on tumour size, lymph nodes, spread, or a combination.
Is the stage confirmed
Sometimes the stage becomes clearer after surgery or further scans.
What does this stage mean for the goal of treatment
Is the aim cure, long-term control, reducing recurrence risk, or symptom relief?
How much does my stage explain, and what else matters
This often opens the door to a more personalised discussion.
Many patients feel flattened by the number attached to their cancer. Stage 4, in particular, can land like a punch. But stage is only one part of the picture. It tells you where the cancer is. It does not tell you everything about how it will behave, how well treatment may work, or how you as an individual will cope.
That’s why the next conversation matters just as much as the stage itself.
Two people can both have kidney cancer and still face very different outlooks. That’s because stage is only the broad framework. Your team personalises prognosis by looking at the biology of the tumour and the health of the person carrying it.
Grade describes how abnormal the cancer cells look under the microscope. Cells that still look more like normal kidney tissue often behave less aggressively. Cells that look very abnormal may be more likely to grow or spread faster. That’s why your pathology report matters, not just your scan result.
Histology means the subtype of kidney cancer. You may hear terms such as clear cell, papillary, or chromophobe. These names aren’t just labels for the lab report. They help doctors estimate behaviour and choose treatments, especially if drug treatment is being considered.
If you’ve seen pathology terms in your report and aren’t sure what they mean, patient-friendly explanations of tests can help. Resources on laboratory medicine can make pathology, biopsy results, and blood markers much easier to understand before your next appointment.
Doctors also look at performance status. That’s a medical way of asking how well you’re managing ordinary life. Are you up and about most of the day? Do you need help with basic tasks? Can you tolerate major surgery or intensive treatment?
Treatment isn’t chosen in a vacuum. The best plan has to fit both the cancer and the person.
Other health conditions also shape prognosis. Kidney function, heart disease, diabetes, high blood pressure, and lung disease can all influence what treatments are safest and how recovery may go. After kidney surgery, preserving as much healthy kidney function as possible can be especially important.
For some people, food planning becomes part of that wider health picture, particularly if kidney function needs monitoring after treatment. Structured meal plans for kidney disease can be useful as a discussion starter with your care team or renal dietitian, especially when you’re trying to balance treatment recovery with kidney-friendly eating.
When kidney cancer has spread, oncologists often use formal risk models to guide treatment discussions. You might hear about blood results, symptoms, and how active you are day to day. These tools don’t replace clinical judgement, but they help doctors group patients into broad risk categories and choose treatment more carefully.
That can feel impersonal at first. In practice, it often means your team is trying to avoid guesswork.
The more specific the information, the more personal the prognosis becomes.
Bring these to clinic if you want a more personalized conversation:
What is the grade of my tumour
Ask what the grade suggests about how active the cancer may be.
What subtype do I have
Different subtypes can behave differently and may respond differently to treatment.
How does my kidney function affect my options
This is especially important if surgery or systemic treatment is being discussed.
What factors about me improve or worsen the outlook
That wording often prompts a more honest and practical answer than asking only for a number.
Patients sometimes compare themselves to someone else online with “the same stage” and panic when the stories don’t match. This is one reason why that comparison can mislead. Their grade may be different. Their subtype may be different. Their age, kidney function, scan findings, and treatment response may all be different too.
A personal prognosis is built from details. That’s why understanding your own report is often more helpful than reading ten strangers’ stories.
A prognosis is based partly on the cancer, but it’s also shaped by what medicine can do about it. Kidney cancer treatment has changed a great deal, and that change matters most when people assume older statistics tell the whole story.
For many patients with localised disease, surgery remains the treatment that offers the best chance of long-term control or cure. That may mean removing the whole kidney, called a radical nephrectomy, or removing only the tumour and a rim of normal tissue, called a partial nephrectomy. When doctors can preserve healthy kidney tissue safely, that can help protect kidney function after treatment.
For some small tumours, doctors may consider ablation rather than standard surgery. Ablation destroys the tumour using heat or freezing. It isn’t right for everyone, but for selected patients it can offer a less invasive option.
The outlook for advanced kidney cancer has also changed because of newer drug treatments. According to Cancer Research UK statistics for kidney cancer survival, net 10-year survival in England is 51%, and overall 5-year survival reached 64% for diagnoses between 2016 and 2020. The same source notes that this improvement is partly linked to treatments introduced after 2009, including tyrosine kinase inhibitors such as pazopanib, which halved the risk of progression in metastatic renal cell carcinoma.
That’s an important reminder. Prognosis is not frozen in time.
Two treatment approaches often come up in kidney cancer care.
Targeted therapy
These drugs act on signals that cancer cells use to grow new blood vessels or continue dividing. Medicines such as pazopanib belong to this group.
Immunotherapy
These treatments help the immune system recognise and attack cancer cells more effectively. They’re now a major part of treatment discussions for many people with advanced clear cell kidney cancer.
If your doctor mentions checkpoint inhibitors or combination treatment, it helps to have a basic overview in plain language. This guide to what immunotherapy is can make those conversations less intimidating.
When people search for kidney cancer prognosis, they often want certainty. Treatment doesn’t offer certainty, but it does shift possibilities. A scan after surgery may show no evidence of disease. A drug may shrink tumours or hold them stable. Side effects may require a treatment change, but another option may still exist.
This is why it’s reasonable to ask not only, “What is my prognosis?” but also:
A prognosis before treatment is only the opening estimate. Response to treatment often tells a more personal story.
That story unfolds over time, through scans, blood tests, symptom changes, and how you feel in yourself.
For many people, the hardest emotional stretch starts after treatment ends. Family members may expect relief, but patients often feel newly exposed. During active treatment, there is a plan. Afterwards, there is waiting.
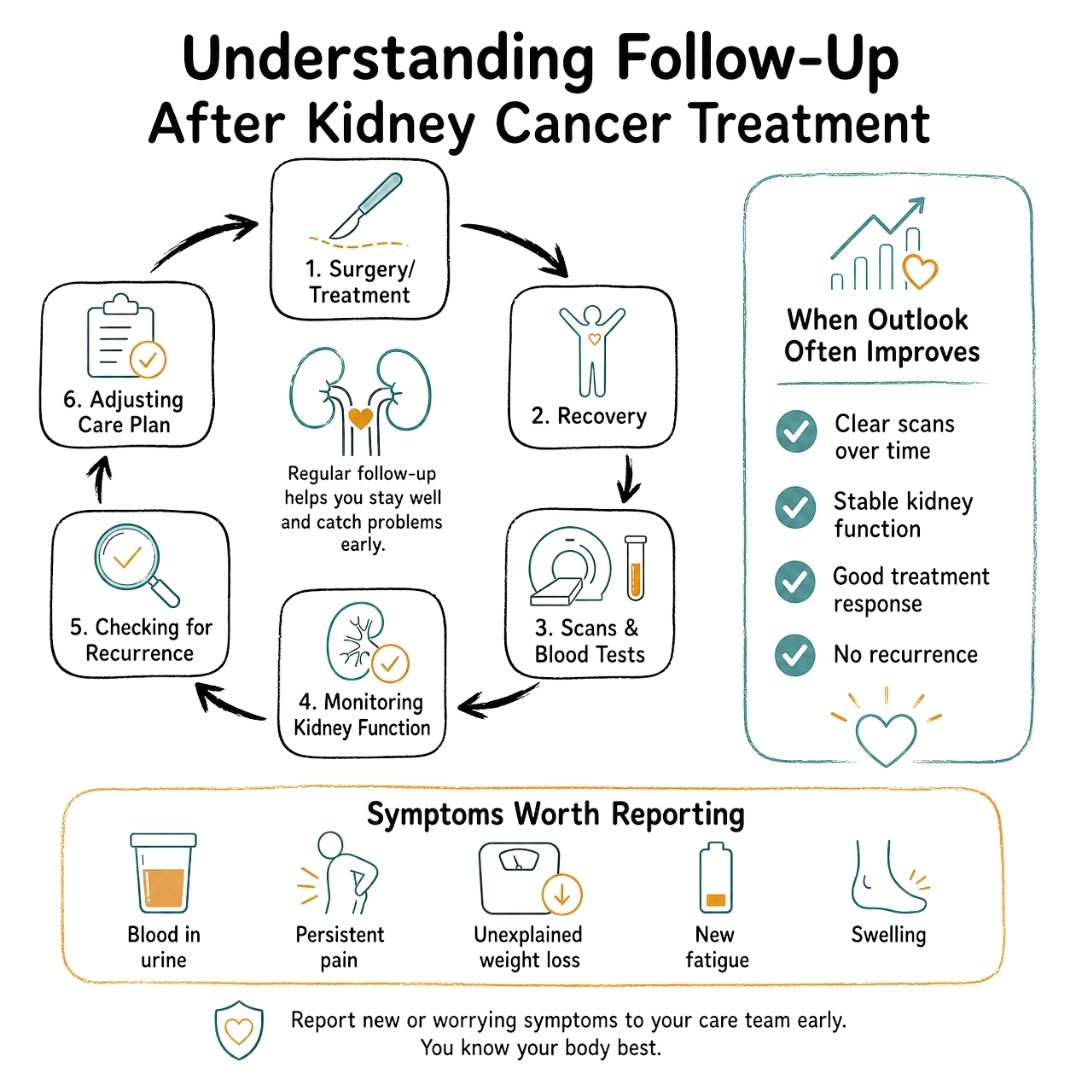
Follow-up care exists to make that waiting safer and more structured.
Doctors use follow-up appointments to look for signs that the cancer has returned, to monitor kidney function, and to manage ongoing effects of treatment. The schedule depends on your original cancer, the treatment you had, and how high or low your recurrence risk appears.
Scans may include CT imaging or other tests, depending on your situation. Blood tests and urine tests may also be part of surveillance. Some appointments focus as much on recovery as recurrence, including blood pressure, renal function, fatigue, pain, and quality of life.
A key point in kidney cancer prognosis is that outlook differs sharply between localised and metastatic disease. Cancer Research UK notes that the 5-year net survival rate is 92 to 95% for localised kidney cancer and 13% for metastatic disease, and that 50% of diagnoses are incidental findings on scans done for other reasons, which often means the cancer is found earlier and treated sooner.
One of the most reassuring ideas in cancer follow-up is conditional survival. This means that if you remain well and cancer-free over time, your future outlook often improves compared with what it looked like at diagnosis.
Patients don’t always hear this clearly enough. The first prognosis you’re given is based on what was known at the start. It can change for the better after successful surgery, clear follow-up scans, or a sustained treatment response.
The longer you do well, the more your doctors can judge your outlook by how you’re doing now, not only by the day you were diagnosed.
These are often more useful than asking for a generic recurrence percentage:
Many people know the phrase “scanxiety” long before they ever hear it in clinic. The days before follow-up imaging can be exhausting. It helps to build routines that keep those weeks from being swallowed by fear.
Some people keep a notebook for symptoms and questions so they don’t spiral every time something odd happens. Others ask for appointment dates well in advance, plan support around scan weeks, or avoid searching online late at night.
If recurrence does happen, it doesn’t mean all options are gone. It means the plan needs updating. That distinction matters.
Statistics can either shut a conversation down or open it up. A lot depends on the question you ask next.
If you hear a survival figure and freeze, try not to leave the appointment there. Numbers become useful when they are translated into something personal, practical, and decision-focused.
Print these, save them in your phone, or hand them to the person coming with you.
You don’t need medical language to ask strong questions. These simple phrases often work well:
Those questions often bring the conversation back to what matters most.
By the end of the discussion, you should have a sense of:
If you leave with only a stage number and a wave of fear, it’s reasonable to ask for another conversation. Good cancer care includes explanation, not just information.
The medical side of kidney cancer prognosis is only part of the story. The human side often takes up more space. Worry about scans, family conversations, work, sleep, money, body image, and the strain of uncertainty can all sit alongside treatment.
Some resources discuss survival well but give little attention to the psychological impact. Yet living with a prognosis often means learning how to carry uncertainty, prepare for follow-up, and protect your mental health at the same time. That gap between medical facts and lived experience is real, as noted in this discussion of the emotional side of prognosis from The Urology Group’s kidney cancer questions guide.
Practical help matters. That may mean lifts to appointments, meal support, someone taking notes during clinic visits, or help sorting insurance and work forms. Emotional support matters just as much. Some people want counselling. Others need peer support, faith support, or a trusted person who can sit with them without trying to fix everything.
Resources that focus on practical support in cancer care and what makes a difference can help patients and carers think beyond treatment alone and identify what lightens the load.
Trusted organisations can also help fill different gaps:
Macmillan Cancer Support
Helpful for practical guidance, benefits advice, and emotional support.
Kidney Cancer UK
Focused information and support for people affected by kidney cancer.
Your hospital team
Specialist nurses, oncology social workers, renal teams, palliative care teams, and psychologists can all play a role.
Hope doesn’t have to mean pretending everything is fine. Sometimes hope is smaller and sturdier than that. Hope is getting a clear explanation. Hope is finding a treatment plan you understand. Hope is knowing who to ring when something changes. Hope is learning that support exists for the parts of cancer that don’t show on a scan.
If you’re looking for added comfort alongside reliable education, Cancer Care Parcel offers evidence-based guides, workshops, and, when funding allows, thoughtfully assembled care parcels for people affected by cancer.
Kidney cancer prognosis can sound like a cold statistic. In real life, it’s a conversation about where you are, what can help, and what matters most to you now. Bring your questions. Ask for plain language. Let your team explain the details more than once if needed. Understanding doesn’t remove the difficulty, but it can return a sense of footing.
We strongly advise you to talk with a health care professional about specific medical conditions and treatments.
The information on our site is meant to be helpful and educational but is not a substitute for medical advice.
Discover Essential Exercise Tips To Stay Active During Cancer Treatment. Learn How To Maintain Strength, Energy, And Well-being With Safe And Effective Activities.
Lorri Lee Shares Her Personal Story As Her Mother Battled Metastatic Breast Cancer. She Shares Tips On How To Cope, As A Loved One Battle Cancer, And Ways To Maintain A Positive Outlook And Lifestyle.
Luis A. Gomez-Sarosi discusses how cancer therapies interact with cancer and non-cancerous cells and the development of early cancer detection methods.
