Let's get straight to the point: no, an ultrasound alone cannot diagnose cancer. Think of it less as a final verdict and more like an expert detective's first look at a crime scene—it’s brilliant for finding clues that tell doctors where to investigate next.

If you've ever seen a submarine movie, you'll know how they use sonar to map the unseen ocean floor. An ultrasound, also called a sonogram, works on a very similar principle for the human body. It uses high-frequency sound waves to create a real-time picture of your organs, tissues, and other internal structures.
During the scan, a trained specialist called a sonographer will glide a small handheld device, the transducer, over the area being examined. This device sends out sound waves which travel into your body, bounce off whatever they meet, and return as echoes. A computer instantly translates these echoes into the black, white, and grey images we see on the monitor.
So, when it comes to investigating a potential cancer, the ultrasound isn't there to give a simple "yes" or "no". Its job is to gather crucial visual evidence about a lump, pain, or other symptom that’s causing concern.
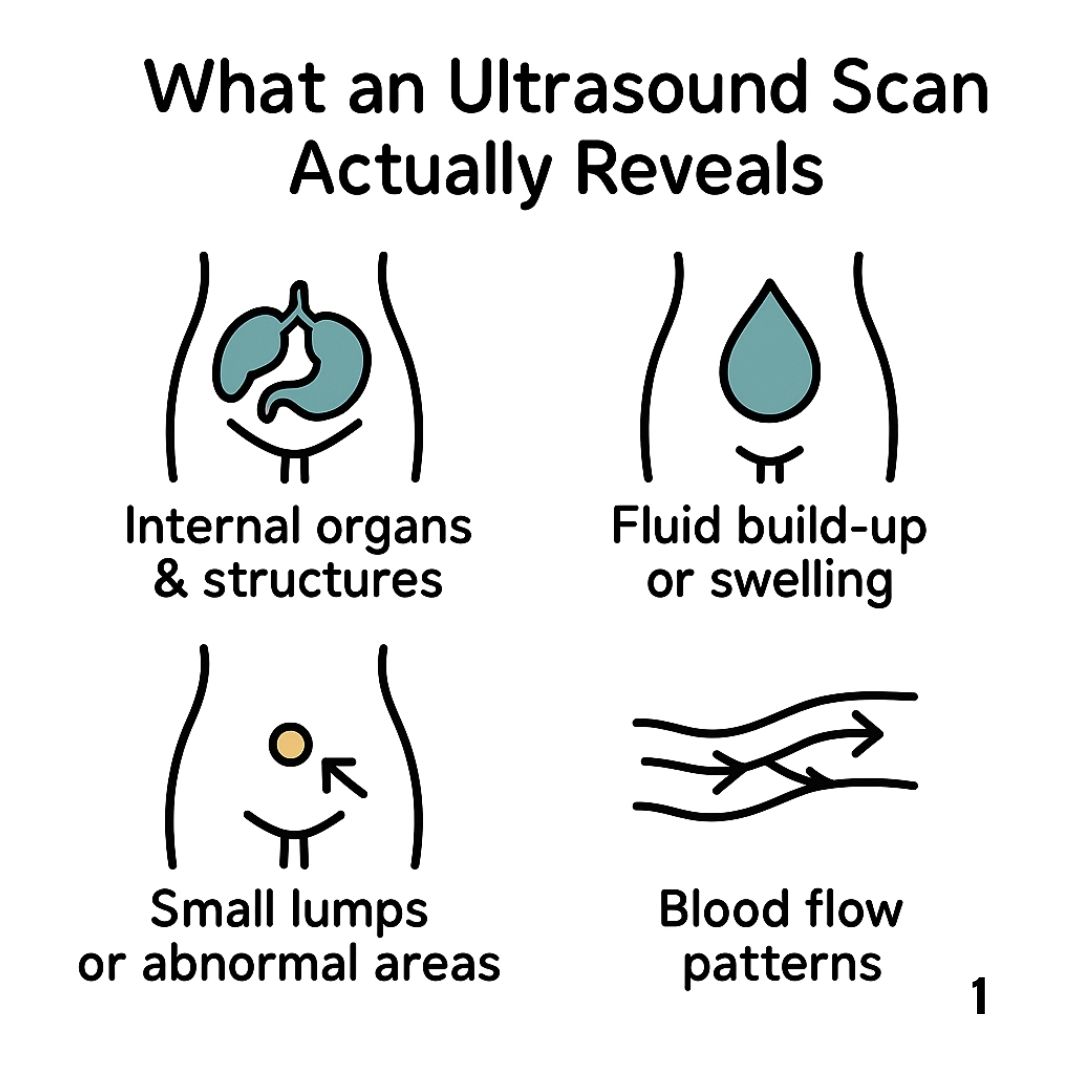
When your doctor refers you for an ultrasound, they’re usually trying to get a better handle on a specific physical finding. The scan is fantastic at showing the physical characteristics of what's going on inside.
Here’s what the sonographer and radiologist are looking for:
This first-pass information is incredibly valuable. Finding a simple, fluid-filled cyst on an ovary or in the breast can bring immediate relief and often means no further tests are needed. On the other hand, finding a solid mass with irregular borders is a clear signal that the investigation needs to go a step further, usually with a biopsy.
An ultrasound doesn't see "cancer." It sees physical structures and their characteristics. A suspicious finding is simply a collection of visual clues that warrant further investigation to rule out or confirm malignancy.
This frontline role is vital. In many countries, initial cancer investigations start with a primary care doctor. For instance, NHS England data shows that for ultrasounds used to check for cancer, 49% were requested directly by GPs, especially for concerns like potential ovarian cancer. This really underlines how essential this tool is in the early diagnostic journey. For anyone going through this, knowing how to ask the right questions can significantly improve your cancer diagnosis experience.
While ultrasound is a versatile piece of kit, there are certain areas of the body where it truly excels. Think of it as the specialist detective called in for cases that need a delicate touch—where its unique skills in seeing soft tissues, telling solid from fluid, and avoiding radiation are most needed. For some investigations, it's the undisputed first port of call.
This is especially true for organs and tissues sitting close to the skin, without bone or gas getting in the way. Sound waves travel through these areas beautifully, giving clinicians a detailed, real-time view that helps them decide on the crucial next steps.
When a lump is found in the breast, an ultrasound is often one of the first tests a doctor will order, frequently working alongside a mammogram. Its biggest strength here is its uncanny ability to distinguish between a fluid-filled cyst (which is almost always harmless) and a solid mass that needs a closer look.
This becomes incredibly important for women with dense breast tissue. A mammogram of dense tissue can be like trying to spot a polar bear in a snowstorm—potential tumours can be hidden. Ultrasound, however, offers a completely different perspective, often clarifying what the mammogram can’t. Recognising this challenge, national research bodies have been developing new ultrasound technologies to better measure breast density, aiming to improve accuracy and catch cancer earlier. You can learn more about this by reading the full case study on new ultrasound technology.
The thyroid gland, right at the front of the neck, is another area perfectly suited for an ultrasound scan. It’s quite common for small lumps, or nodules, to grow on the thyroid, and thankfully, the vast majority are benign.
An ultrasound gives an incredibly detailed picture of these nodules, letting a radiologist check for features that might hint at a higher risk of cancer. They'll look at a few key things:
Based on what they see, doctors use a scoring system to decide whether to simply keep an eye on the nodule or perform a fine-needle biopsy to get a definitive answer.
Ultrasound is a cornerstone of gynaecological health, routinely used to get to the bottom of symptoms like pelvic pain, bloating, or unusual bleeding. It provides a clear window into the uterus, ovaries, and nearby structures.
A transvaginal ultrasound, for instance, uses a small probe to get incredibly detailed images of the ovaries. This is vital for checking ovarian cysts or masses that could be linked to ovarian cancer. In the same way, it can measure the thickness of the uterine lining (the endometrium), a key early indicator for uterine cancer.
In the pelvic region, ultrasound acts as the first-line investigator. It can quickly spot structural problems, guide the need for further tests, and often provide immediate reassurance by ruling out the most serious concerns.
For men, an ultrasound is the go-to method for checking a lump or swelling in a testicle. It can easily tell if a mass is inside the testicle itself—a key sign of testicular cancer—or if it's something separate and less worrying, like a cyst.
It’s also used to guide biopsies of the prostate gland. While a PSA blood test or a physical exam might raise a red flag, a transrectal ultrasound (TRUS) lets a urologist actually see the prostate and take precise tissue samples for analysis. Knowing that early detection is key to prostate cancer survival really highlights how important these follow-up procedures are.
The table below gives a quick summary of how ultrasound is typically used across different parts of the body when cancer is a concern.
| Area of Body | What Ultrasound Helps Identify | Typical Next Step if Abnormal |
|---|---|---|
| Breast | Differentiates solid masses from fluid-filled cysts, especially in dense tissue. | Biopsy (e.g., core needle biopsy) of the solid mass. |
| Thyroid | Characterises nodules (size, shape, composition) to assess cancer risk. | Fine-needle aspiration (FNA) biopsy for suspicious nodules. |
| Ovaries/Uterus | Evaluates ovarian masses and measures uterine lining thickness. | MRI, blood tests (e.g., CA-125), and potential biopsy. |
| Testicles | Determines if a lump is inside the testicle (suspicious) or outside. | Surgical removal of the testicle (orchiectomy) for diagnosis and treatment. |
| Prostate | Guides needles to take tissue samples from suspicious areas. | Further analysis of biopsy samples to confirm cancer and determine its grade. |
| Liver/Kidneys | Detects tumours, cysts, or lesions that could indicate cancer. | CT scan, MRI, or a targeted biopsy for a definitive diagnosis. |
This shows that while ultrasound is rarely the final word, it's an indispensable guide that points specialists exactly where they need to look next.
Finally, ultrasound is a workhorse for examining abdominal organs like the liver, gallbladder, pancreas, and kidneys. It’s excellent for spotting tumours or other abnormalities. For example, if blood tests reveal poor liver function, an ultrasound is a fast and effective way to check for lesions that might point to liver cancer, particularly for patients with risk factors like cirrhosis.
When a radiologist looks at your ultrasound, they don't see a simple "cancer" or "not cancer" label. Think of them as interpreters, fluent in a complex visual language of greyscale shapes, shadows, and textures. Their skill lies in translating these patterns into a medical assessment, sifting through the images to separate harmless findings from anything that needs a closer look.
It’s a bit like a jeweller examining a gemstone. To an untrained eye, two stones might look much the same, but the expert instantly spots the subtle details—the clarity, cut, and internal flaws—that reveal its true nature. In the same way, a radiologist meticulously analyses every feature of a lump or lesion to build a picture of what it could be.
So, what are they actually looking for? Let's start with something straightforward, like a simple, benign cyst. On an ultrasound, this usually appears as a perfectly round or oval shape with smooth, clean borders. It's like a tiny water balloon: predictable, uniform, and neatly contained. Because it’s full of fluid, sound waves pass straight through it, creating a dark, empty space (what we call anechoic) on the scan. These are all reassuring signs.
A potentially malignant mass, however, often tells a very different story. Its structure can look chaotic and disorganised. Instead of those smooth edges, it might have irregular, jagged, or even spiky borders that seem to push their way into the surrounding tissue. This kind of invasion suggests the growth isn't respecting the body's normal boundaries.
Here are the key visual clues that can raise a red flag for radiologists:
These are just a few pieces of the puzzle. It’s the combination of these features that helps the radiologist to categorise a finding and decide what needs to happen next.
Beyond just shape and texture, radiologists have another powerful tool in their arsenal: Doppler ultrasound. This special setting lets them see and measure blood flow within a specific area. It works a bit like a weather radar detecting wind speed, but instead of tracking air currents, it follows the movement of red blood cells through vessels.
This is a critical piece of information. Why? Because malignant tumours often need to create their own blood supply to keep growing—a process known as angiogenesis. A benign lump, on the other hand, typically has very little internal blood flow, if any at all.
If a solid mass shows a rich and disorganised network of blood vessels running through it, this is considered a significant red flag. It suggests the mass is actively building a supply line to fuel its growth, a hallmark of malignancy that strongly signals the need for further investigation.
Seeing these suspicious signs on an ultrasound is what triggers the next diagnostic step. For a breast abnormality, this almost always means getting a tissue sample. You can learn more about how specialists do this in our detailed guide to a stereotactic breast biopsy. It’s this next step—the biopsy—that provides the definitive answer an ultrasound alone cannot.
While ultrasound is a fantastic first-line tool for looking inside the body, it’s important to have an honest picture of what it can and can't do. Knowing its limitations helps set realistic expectations and explains why it’s almost always part of a team of diagnostic tools, rather than a solo act.
The quality of an ultrasound scan hinges massively on the person performing it. A sonographer’s experience and technique are what make the difference between a fuzzy, inconclusive picture and a clear, detailed image that a radiologist can confidently interpret. In short, the image is only ever as good as the person who captured it.
On top of that, ultrasound has its physical limits. Sound waves travel brilliantly through soft tissues and fluids, but they hit a wall—literally—when they encounter bone. They also get scattered by air. This makes ultrasound unsuitable for looking at organs shielded by bone, like the brain, or getting a clear picture of air-filled structures like the lungs or most of the bowel.
To really get to grips with ultrasound's role, we need to understand two key ideas: sensitivity and specificity.
Think of it like using a metal detector on a beach.
Ultrasound is generally highly sensitive; it’s excellent at spotting that something is there. The flip side is that its specificity can be lower, meaning not every lump or lesion it picks up is cancer. This can lead to "false positives"—where a scan flags something that turns out to be harmless, causing a lot of worry and triggering more tests.
A "suspicious" finding on an ultrasound is not a diagnosis. It's simply a signal that more information is needed. The high sensitivity ensures potential problems aren't missed, while follow-up tests provide the specificity needed for an accurate diagnosis.
This trade-off is common in medical imaging. For example, a major study on ovarian cancer screening, the UKCTOCS trial, gave us some solid data on this. In the trial, ultrasound screening detected about 68.5% of ovarian and tubal cancers within a year, which shows good sensitivity. Its specificity was incredibly high at 99.7%, yet the chance that a positive test actually meant cancer was just 11.8%. This shows that while most positive findings weren't cancer, they correctly prompted further investigation. You can discover more insights about these ultrasound findings in the UKCTOCS trial.
A person’s own body can also influence how well an ultrasound works. In individuals with a larger body size, for instance, the sound waves have more tissue to get through to reach an organ. This can weaken the returning echoes and lead to less clear, or "attenuated," images. Scar tissue from past surgeries can also sometimes distort the sound waves, making the images trickier to interpret.
Because of these built-in limitations, a suspicious finding on an ultrasound is rarely the end of the story. It's the starting point that points your healthcare team toward the right next steps. The journey from that first scan to a definite answer often brings in other tools and specialists, including more advanced imaging and the critical field of laboratory medicine, which provides the final, cell-level analysis needed to diagnose cancer.
While ultrasound is a go-to for initial investigations, it’s just one of several imaging techniques doctors use. Each one has unique strengths and is suited for different situations.
This table gives a quick rundown of how ultrasound stacks up against other common imaging methods.
| Imaging Technique | Best For | Key Limitations | Uses Radiation? |
|---|---|---|---|
| Ultrasound | Soft tissues, cysts vs. solid masses, guiding biopsies, real-time imaging | Operator dependent, blocked by bone/air, less detail in larger patients | No |
| CT Scan | Detailed cross-sections of bones, tissues, and blood vessels; staging | Higher radiation dose, less effective for some soft tissue detail, contrast dye risks | Yes |
| MRI | Exceptional soft tissue detail (brain, spine, joints, abdomen), staging | Expensive, time-consuming, noisy, not suitable for patients with certain metal implants | No |
| PET Scan | Detecting metabolic activity in cells, finding cancer spread (metastasis) | High radiation dose, less anatomical detail, can have false positives from inflammation | Yes |
As you can see, no single scan does it all. A doctor's choice of imaging depends on the type of cancer suspected, its location, and what specific question they need to answer—whether it's finding a lump, checking its features, or seeing if it has spread. Often, the most complete picture comes from combining these different views.
Getting the news that your ultrasound was abnormal or "suspicious" can be a deeply unsettling moment. It’s natural to feel a rush of uncertainty, but understanding what comes next can help you feel more in control. It's crucial to remember that an unusual scan isn't a diagnosis; it’s simply a green light for a closer look.
Think of it this way: your healthcare team now has a specific area to focus on. Their goal is to gather more detailed information to figure out exactly what the ultrasound picked up. This is a methodical process, and every step is designed to bring you closer to a clear answer.
The first thing that happens after your scan is a radiologist—a doctor who is an expert at reading medical images—writes a detailed report. This report is then sent to the clinician who originally referred you for the ultrasound.
The report will use specific medical terms to describe the findings, noting the size, shape, location, and other features of anything unusual they spotted. Your doctor will then sit down with you to translate this report into plain English, explaining what it means for your health.
Often, the most logical next step is to get a different kind of picture. Ultrasound is a fantastic first-look tool, but other imaging techniques can provide a different perspective and show details that sound waves can't capture.
Your doctor might suggest one of the following:
These scans essentially create a more complete map of the area, helping your medical team plan the best course of action.
While imaging tests provide vital clues, they are still just showing shadows and shapes. The only way to know for certain if a mass is cancerous is to look at the cells under a microscope. This is done through a procedure called a biopsy.
A biopsy involves taking a very small tissue sample from the suspicious area. A pathologist then analyses this sample in a lab. The procedure is often guided by imaging, like ultrasound or CT, to ensure the needle gets to the exact right spot.
A biopsy is the definitive step. It moves beyond asking, "Does an ultrasound show cancer?" to providing a concrete answer to the critical question, "Are these specific cells cancerous?"
The results will confirm if cancer is present. If it is, the biopsy also reveals crucial information about the type of cancer and its characteristics, which is essential for planning any treatment.
This decision tree infographic shows how various factors can influence ultrasound results and why further tests are often needed.
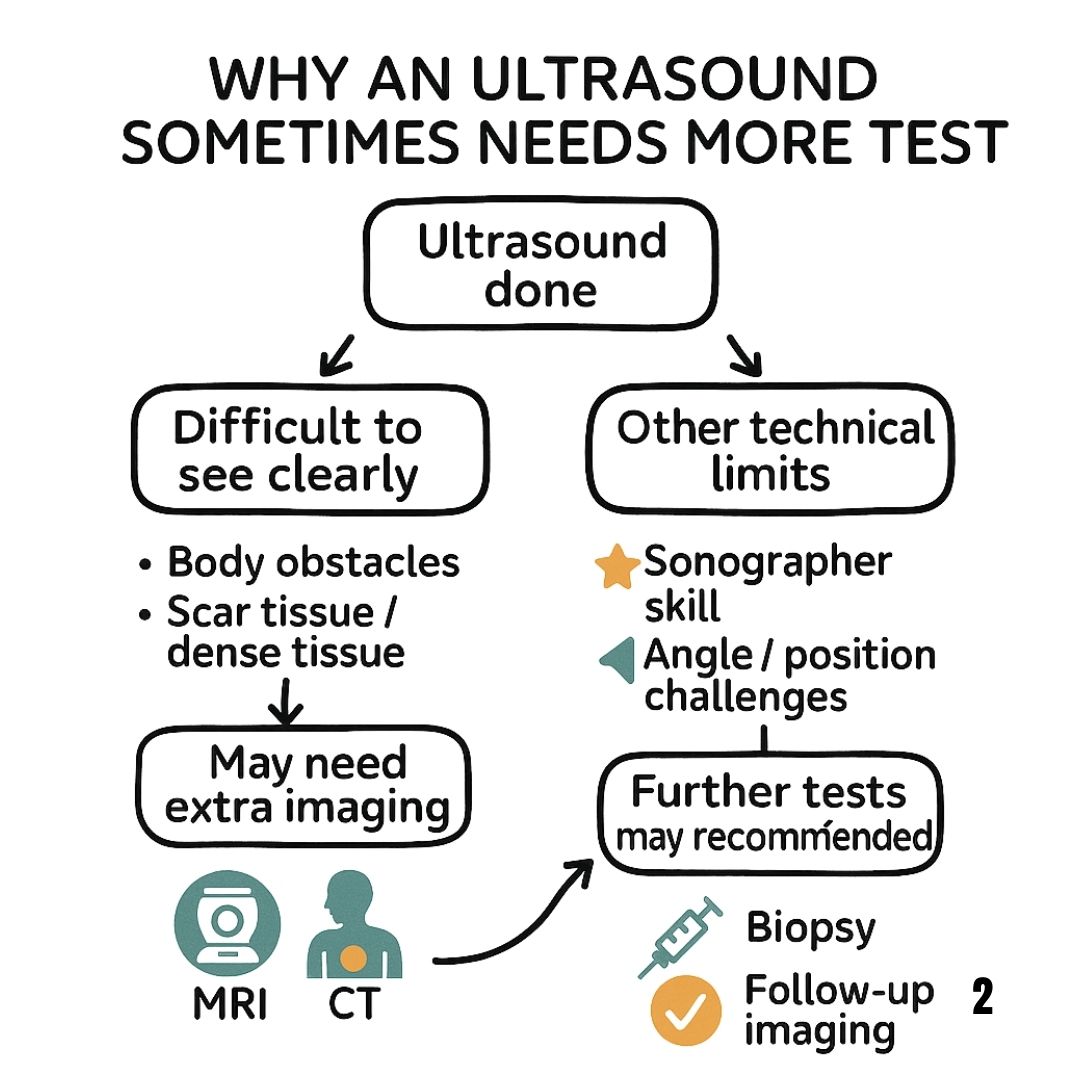
As you can see, the journey doesn't just stop with one scan. The sonographer's expertise and even physical factors are why follow-up tests are a standard, necessary part of getting a reliable diagnosis.
If a biopsy confirms a cancer diagnosis, your care will be managed by a team of specialists, often known as a multidisciplinary team (MDT). This team typically includes surgeons, oncologists (cancer doctors), specialist nurses, and other experts who work together to create a treatment plan tailored just for you.
This can be an incredibly emotional time, but you are not on your own. Learning what to do when you find out you have cancer can help you process the news and take an active role in your care. Remember, there is a clear path forward, and each test is another step towards getting the answers and the support you need.
It's completely normal to have a million questions running through your head, especially when you're waiting for tests and results. That period of uncertainty can be tough. So, let's clear up some of the most common queries people have when an ultrasound is part of their health journey.
Think of this as a practical guide to help you feel more prepared and informed for the conversations ahead with your healthcare team.
Yes, unfortunately, an ultrasound can miss cancer. Its accuracy really hinges on a few things: the skill of the person performing the scan (the sonographer), the type of cancer and where it’s located, and even your own body's unique characteristics.
For example, very tiny tumours might simply be too small to show up clearly. Growths can also be hidden behind organs filled with air, like the bowel, which essentially creates a blind spot because sound waves can't travel through gas. That's why an ultrasound is almost always just one piece of the diagnostic puzzle, not the final word. If your symptoms don't go away after a "clear" scan, it’s vital to go back to your doctor and keep the conversation going.
The timeline for getting your results can vary. Once the scan is done, a radiologist—a doctor who specialises in reading medical images—will carefully analyse the pictures and compile a formal report. That report is then sent to the doctor who originally referred you.
If the findings look urgent, this whole process can be fast-tracked, and your doctor might get the report in a day or two. For more routine scans, it usually takes about one to two weeks before you have a follow-up appointment to discuss what they found. Never be afraid to ask the clinic for a rough timeframe when you’re having your scan.
A Quick Note on Terminology: If you see the word "suspicious" on an ultrasound report, please don't jump to the worst conclusion. It is not a diagnosis of cancer. It’s simply a medical term that means an area has features that need a closer look—usually with a biopsy—to figure out exactly what’s going on. Many benign things can look suspicious on a scan.
This is such a critical distinction. The term just flags that more certainty is needed, and only a more definitive test can provide that.
Walking into your follow-up appointment feeling prepared can make a world of difference. Jotting down a list of questions beforehand means you won’t forget something crucial during what can be a stressful conversation.
Here are a few key questions you might want to ask:
Bringing a notepad or having a trusted friend or family member with you can be a huge help. They can take notes and give you support, helping you feel more in control.
No, absolutely not. This is probably the most important thing to take away. The word "suspicious" just means a finding has features that warrant a closer look to be sure. Think of it as a signal for more investigation, not a final verdict.
Loads of completely benign (non-cancerous) conditions can look "suspicious" on an ultrasound. These include things like:
The whole point of flagging something as suspicious is to be thorough and make sure nothing is missed. It’s what triggers the necessary follow-up—most often a biopsy—which is the only way to get a conclusive answer. The scan raises the question; the biopsy gives the answer.
We strongly advise you to talk with a health care professional about specific medical conditions and treatments.
The information on our site is meant to be helpful and educational but is not a substitute for medical advice.
The bruised cervix guide discusses causes, symptoms and effective relief. Learn prevention tips and expert advice for cervical health.
Discover What Lung Cancer Treatment Looks Like in 2025, From Cutting-Edge Research and Targeted Therapies to Practical Tips and Emotional Wellbeing.
This new YouTube review is from the popular lifestyle blog "Alejandra's Life"
