When a nurse says, “We’ll need to put a cannula in your arm,” many people hear only that one word, "cannula", and stop taking in the rest. Instantly, your mind might jump straight to asking these questions: Will it hurt? How long will it stay in? What if they can’t find a vein?.
That reaction is completely normal.
If you’re having cancer treatment, a cannula in the arm is one of the most common procedures you’ll come across. It may be routine for the medical team, but it rarely feels routine when it’s your body, your treatment day, and your anxiety sitting right there with you. The good news is that once you understand what a cannula is, what it’s used for, and what to look out for, it usually feels far less mysterious.
You’re sitting in a treatment chair. Maybe you’ve brought a book but can’t concentrate on it, or perhaps someone is sitting with you, or maybe you’re doing your best to look calm on your own. Then a nurse smiles and says you’ll need a cannula before your medicines can start.
That small moment can feel much bigger than it sounds.
A cannula is a standard medical tool, but for patients it often represents something more. It can mean treatment is becoming real. It can remind you of earlier hospital visits. If you’ve had difficult blood tests or past failed attempts, the thought of it might make you feel tense before anyone even opens the dressing pack.
A cannula is not just a plastic tube. For many patients, it carries a lot of emotional weight. It can trigger worries about pain, loss of control, and the fear of hearing, “We’ll need to try again.” That’s especially true if you’re already managing fatigue, nausea, or the stress of learning about what chemotherapy is.
You are not being difficult if you feel nervous about a cannula. You are simply having a human response to a medical procedure during an already difficult time.
There are a few simple things that can make the first moments with a cannula easier:
One of the most common misunderstandings is about the needle. The needle does not stay in your arm. It’s only used to guide the cannula into place. Once the cannula is positioned, the needle is removed, leaving a soft plastic tube behind.
That single detail reassures many patients and helps them feel more at ease.
A cannula is a small, soft, flexible plastic tube that is gently placed into a vein, usually in the hand or arm. The easiest way to think about it is as a temporary doorway into your bloodstream. Once it’s in place, your healthcare team can give treatment through that doorway, without needing to insert a new needle each time.
For cancer care, that can be very useful. A cannula may be used to give fluids, anti-sickness medicines, chemotherapy, antibiotics, or pain relief, or even to take blood samples, all through the same access point, depending on your treatment plan. This helps make the process smoother, safer, and less uncomfortable for you.
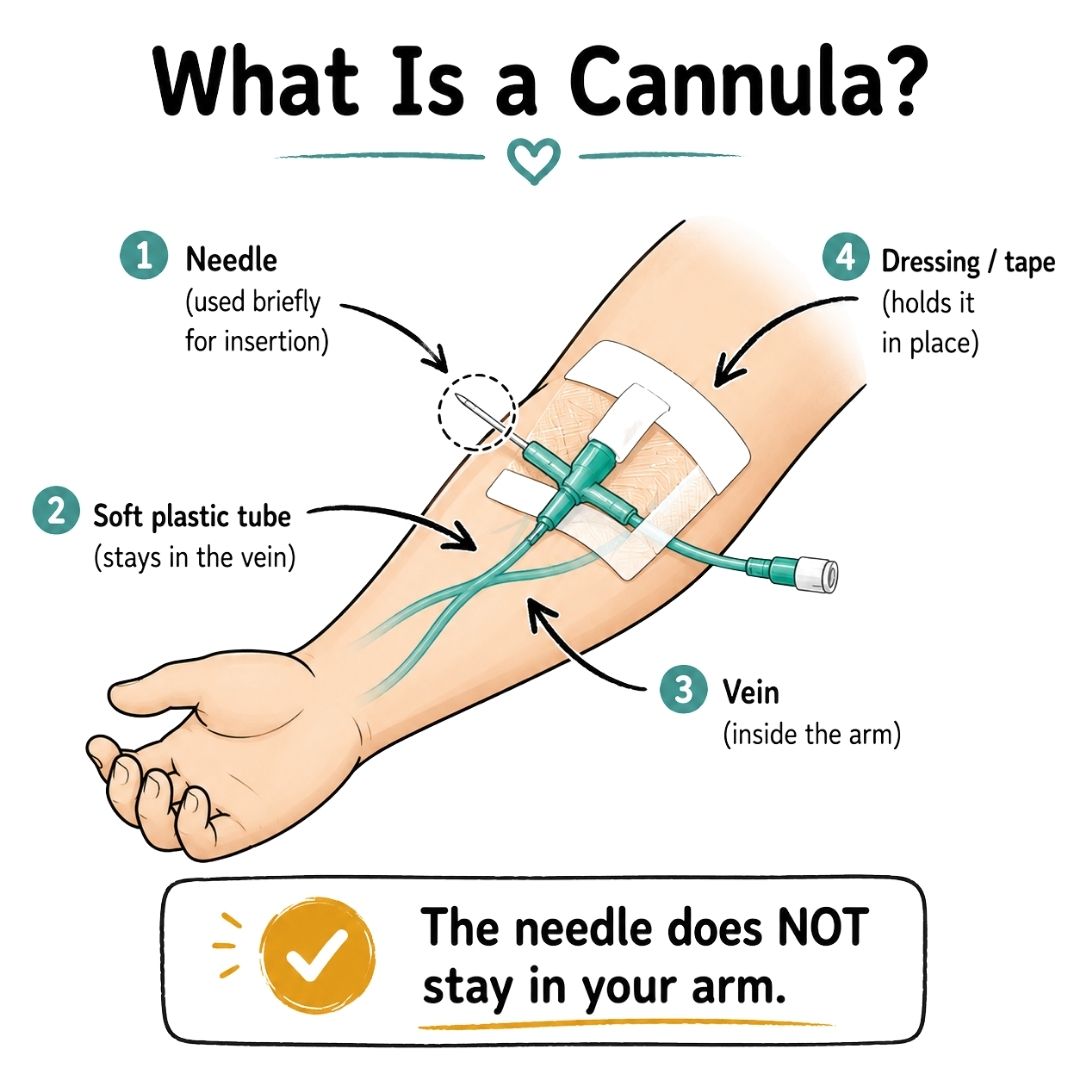
Think of your vein as a hallway and the cannula as a small, secure door that healthcare staff can open whenever treatment is needed. Without it, every medicine or fluid would require another needle puncture. With it, treatment can often be given more smoothly. This makes the whole process gentler on your veins and often more comfortable for you.
That doesn’t mean every patient will use a standard arm cannula for every stage of care. As treatment progresses, some people later need a PICC line, port, or midline. But for many appointments, a basic cannula in the arm is the starting point.
Cannulas come in different gauges, which means different sizes. Your nurse doesn’t choose the size at random. They select the size based on your treatment needs and the vein being used.
Clinical guidance indicates that:
It’s important to remember that a bigger cannula is not automatically better. The right cannula is the one that fits the vein, suits the treatment, and is most likely to work comfortably without causing unnecessary discomfort.
Here’s why having a cannula can make your treatment day easier:
Practical tip: If you’re ever unsure why a particular cannula size or site has been chosen, ask. Patients have every right to understand what’s going into their own arm and why.
Cannula insertion is often quick. For many patients, the difficult part is often the waiting and anticipation beforehand. Once you know the sequence, it tends to feel less daunting.
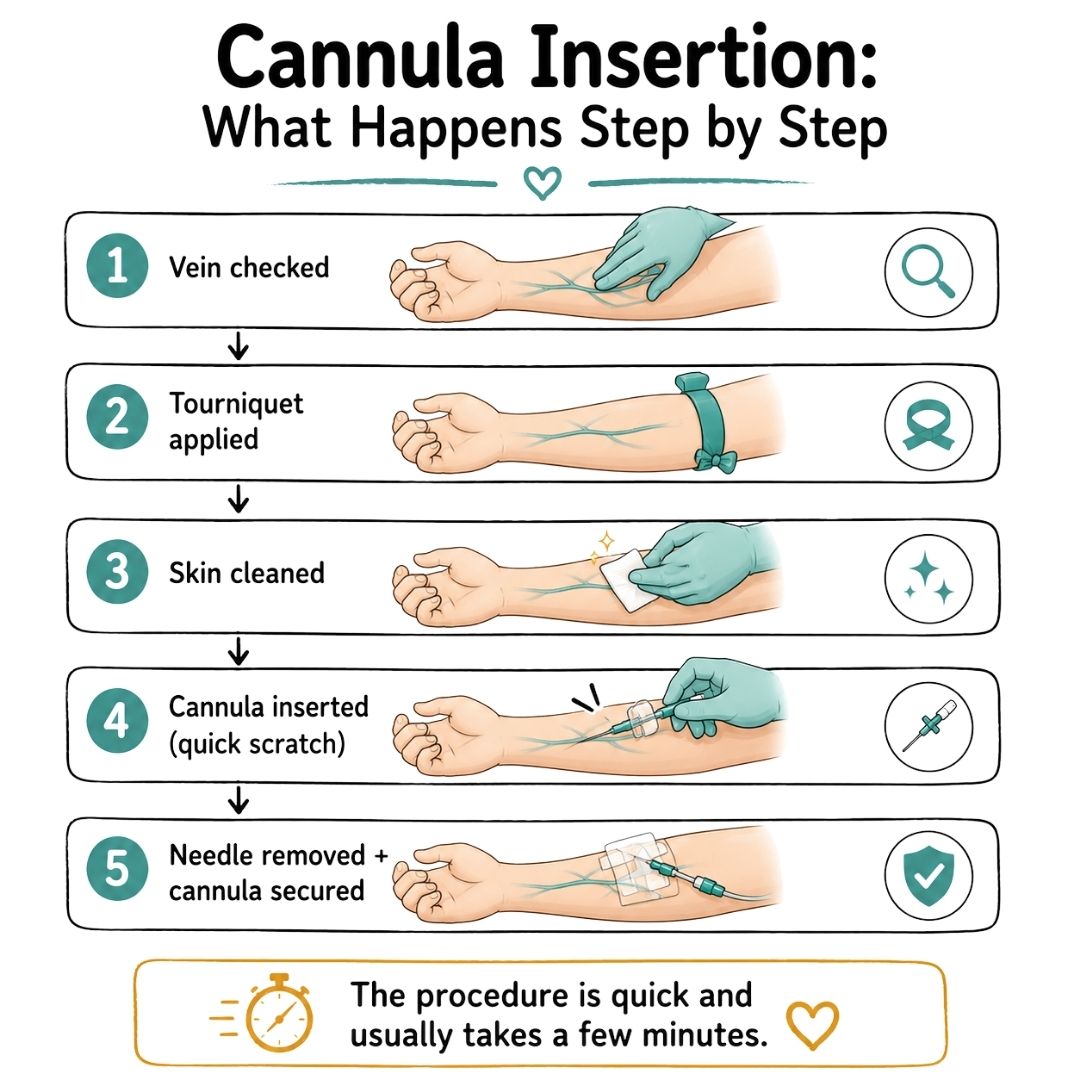
A nurse or clinician will usually examine your hand, wrist, or forearm to find a suitable vein. They may choose your non-dominant arm if possible, though the best vein matters more than a fixed rule. A tourniquet goes on first. That’s the tight band that makes the veins easier to see and feel.
Next, the skin is cleaned with an antiseptic, which often feels cool. The clinician will then steady your arm and let you know to expect a brief, sharp scratch as the cannula is inserted.
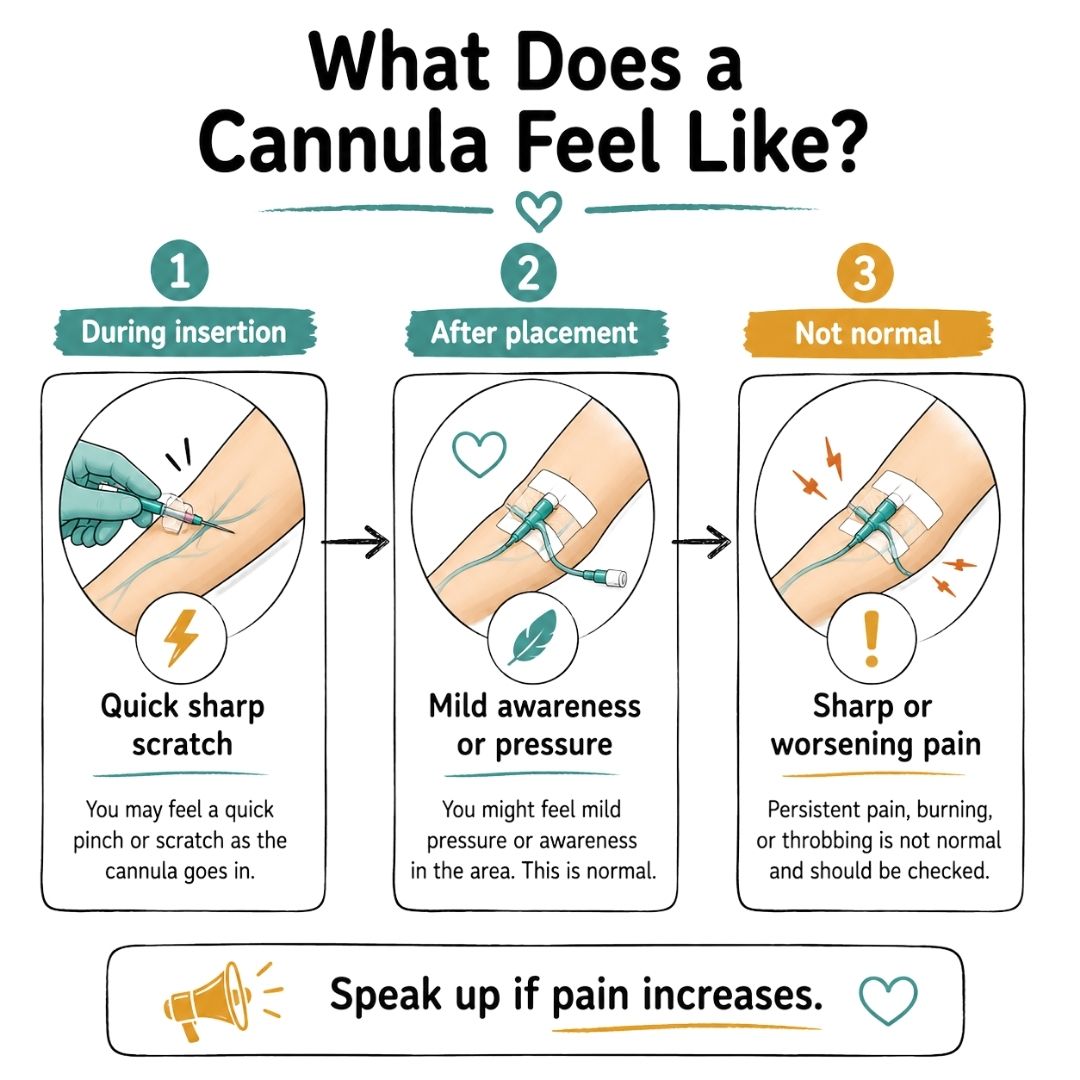
The needle part is brief. Many patients describe it as a sting or pinch that settles quickly. After that, the soft plastic tube stays in place, and the needle comes out.
Once the cannula is secured with a clear dressing or tape, you may feel some awareness of it, but you shouldn’t feel sharp pain. A little tenderness or pressure is normal.
If you do feel strong or increasing pain, speak up straight away; that’s important information for the team.
If you’re preparing for your first chemotherapy session, it can help to know that nurses perform this procedure frequently and will usually talk you through it as they go.
This is the part many leaflets tend to underplay, but patients often remember it very clearly.
Clinical studies have found that first-time insertion success rates are around 73% for peripheral cannulas. The remaining 27% required more than one attempt, with 15% requiring a second attempt and 9% requiring three or more attempts. A small percentage (3%) had no recorded number of subsequent attempts. based on published clinical research.
This matters because if a first attempt doesn’t work, it does not mean you’ve done something wrong. It may reflect small veins, dehydration, scarred veins, cold hands, previous treatment, or a tricky angle on the day.
If nurses need another attempt, you’re allowed to pause, breathe, ask who else can try, or ask whether a more experienced clinician or ultrasound-guided insertion is available.
Here are simple steps that can make cannula insertion go more smoothly:
The procedure is simple. But the experience can still be emotional. Both realities can exist at the same time, and acknowledging that often makes the process easier.
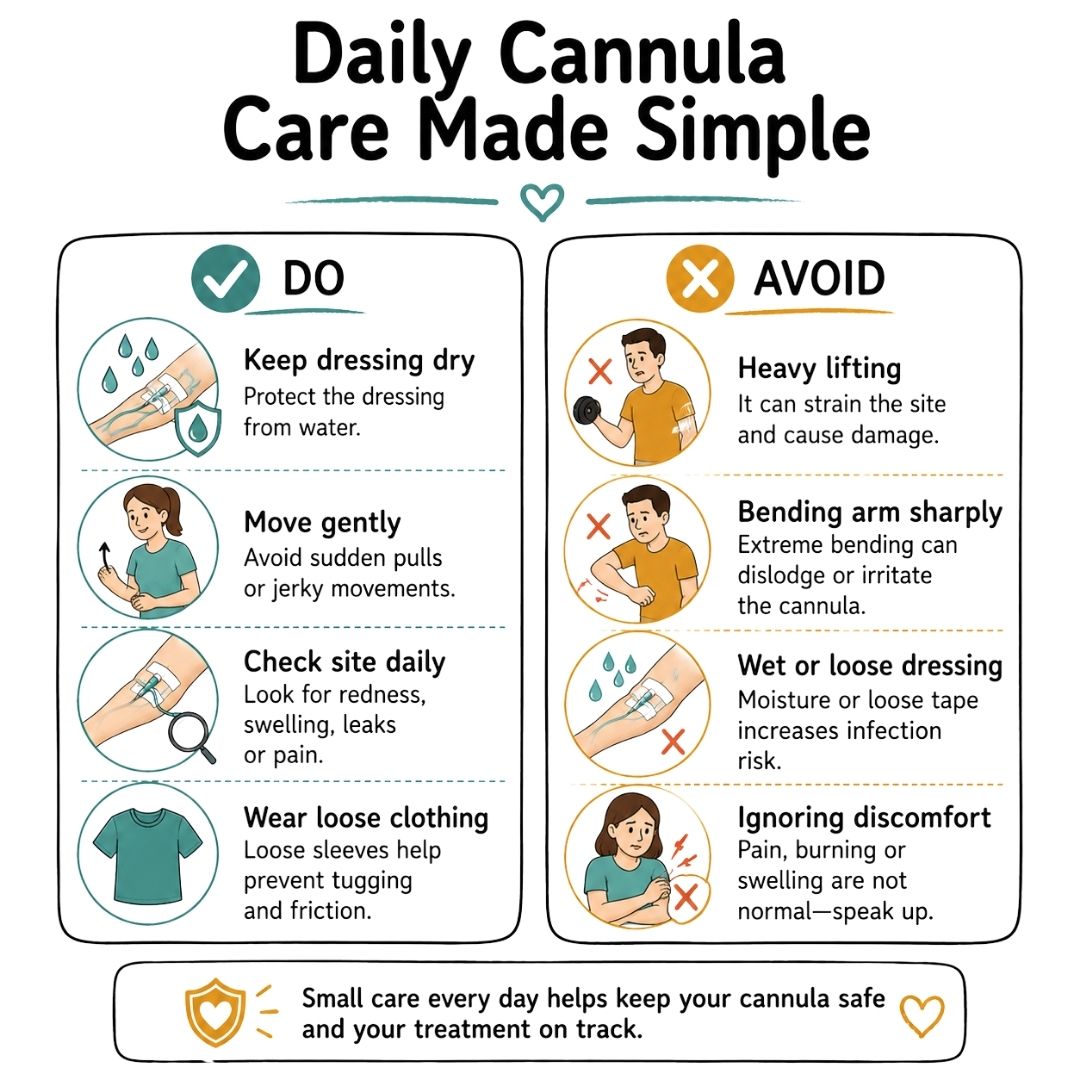
Once the cannula is in, patients are often relieved to find that it’s less dramatic than they feared. You can usually move your arm, hold a cup, use your phone, and get around normally. The main goal is to avoid knocking it, bending it sharply, or soaking the dressing, as these can cause discomfort or affect how well the cannula works.
The best approach is gentle common sense. Here are some practical tips to help you feel more comfortable while living with a cannula:
A glance at the cannula site can prevent problems later. You don’t need to inspect it obsessively. Just build a simple habit.
Ask yourself:
If the answer to any of those changes suddenly, let a nurse know.
A cannula should fit into your daily life as much as possible without taking over it. If you find yourself protecting it every second or avoiding normal movement because it hurts, that's a sign it needs checking.
| Do | Why it helps |
|---|---|
| Tell staff if it snags or pulls | A cannula can shift without fully coming out |
| Use the other arm for heavier tasks | This reduces irritation at the site |
| Carry useful comfort items | Tape-friendly clothing and small essentials help on long clinic days |
| Ask before covering it with creams | Some products can loosen dressings |
If you’re packing for a long appointment, a few ideas in this guide on what to pack in a chemo bag can make the day more manageable.
Most cannulas work without major issues, but problems are easier to fix when they’re noticed early. The key is knowing what signs to look out for.
A prevalence survey reported phlebitis in 4.69% of patients with arm cannulas and infiltration in 3.35%, according to this prevalence survey on peripheral intravenous catheter complications. Those figures are not there to frighten you. They’re a reminder that site checks matter.
It’s important to know what changes to watch for. Contact your treatment team if you notice any of the following:
Other signs to take seriously include:
Some medications, including certain chemotherapy drugs, require careful monitoring during infusion, which is why reporting pain or burning immediately is so important.
Don’t wait to see if discomfort settles on its own or if the area is becoming more painful or visibly changing.
Safety reminder: Sharp pain, swelling, or burning during an infusion is never something to sit through quietly. Always let your healthcare team know.
Basic hygiene matters more than fancy products. Always clean your hands before touching the dressing, avoid picking at the tape, and don’t ignore small changes just because you don’t want to “bother” anyone.
If you want a broader overview of effective infection prevention advice, this guide is useful for understanding why clean technique and early reporting matter in healthcare settings.
If your skin is already dry, fragile, or sensitive from treatment, extra skin care around the surrounding area can help. Resources on healing and protecting skin may be useful alongside the advice you receive from your care team.
A standard cannula in the arm is often the simplest and most common option, but it isn’t always the right fit for everyone. If your veins are difficult to access, your treatment is expected to run over a longer period, or repeated insertions have become physically and emotionally distressing, your medical team may suggest another type of access device.
The three terms patients most commonly hear are:
Each option has its own role depending on your treatment needs. You may also hear about a midline catheter, which sits somewhere between a standard cannula and a PICC line.
Some patients manage well with a new cannula at every treatment session. Others reach a point where every appointment begins with worry about whether the team will be able to get access at all. When this happens, the conversation often shifts from “Can we get a cannula in today?” to “What’s the best longer-term plan?”
In the UK, some NHS trusts use midline catheters for patients who need access for up to 30 days. These are inserted in the upper arm with ultrasound guidance. Midlines may reduce vein damage, lower the risk of deep vein thrombosis (DVT), and cut infection rates compared with PICC lines, according to the procedural guide to midline insertion.
| Feature | Peripheral Cannula | PICC Line | Port (Port-a-Cath) |
|---|---|---|---|
| Where it sits | Hand or arm vein | Upper arm, with a longer tube into a larger vein | Under the skin, usually in the chest |
| How long has it been used | Short-term | Longer-term treatment | Longer-term treatment |
| How it’s inserted | Bedside procedure | Specialist placement | Minor procedure |
| Visible outside the body | Yes | Yes | No, except when accessed |
| Best for | Short appointments or short courses | Repeated treatment and poor peripheral access | Ongoing maintenance as advised by the team |
| Day-to-day care | Basic dressing checks | Regular flushing and dressing care | Ongoing maintenance as advised by team |
The right question isn’t “Which device is best? ” but rather “Which device best matches my treatment and veins?”
If repeated failed attempts are starting to affect your confidence, say so directly. Emotional strain is a valid clinical issue, not a side note. If cancer treatment has made you feel as though your body is no longer your own, support for that feeling matters too. Some people find it helpful to read about the emotional side of treatment changes, including reflection on space invader fallout, which explores how medical experiences can linger in the mind long after the appointment ends.

No. The needle is used to place the cannula, and then it is removed. What stays in your vein is a soft plastic tube.
Yes. Many cancer patients experience difficult peripheral intravenous cannulation, often because treatment makes veins more fragile. That can cause real anxiety, and it’s often not addressed clearly enough in patient information, as noted in this NHS cannula care resource.
Be direct and specific. Tell staff if you’ve had multiple failed attempts, if one arm tends to be better, if you’re frightened of needles, or if you’d like the most experienced person available.
Useful questions include:
Yes. You can ask for a pause at any time. You can ask what the plan is before another attempt goes ahead.
If you cry, that’s completely okay and more common than people expect.
Plenty of calm, capable adults cry during cannulation, especially after repeated procedures. Tears do not mean you’re weak or failing to cope.
Trust your instincts and don’t hesitate to get help if something doesn’t feel right. Contact your treatment team or go to urgent care straight away if you notice any of the following:
It’s always better to check early than to wait and hope it improves. Your team would much rather you spoke up than risk a complication.
A cannula may be small, but your experience around it can be significant. It’s completely normal to feel anxious, frustrated, or even overwhelmed by something that medical staff do many times a day.
If you’re supporting someone through treatment or going through it yourself, practical guidance can make those moments feel less frightening and less lonely. For more patient-friendly cancer support, comfort ideas, and educational resources, visit Cancer Care Parcel.
We strongly advise you to talk with a health care professional about specific medical conditions and treatments.
The information on our site is meant to be helpful and educational but is not a substitute for medical advice.
Feeling overwhelmed? This practical guide shows you how to prepare for chemotherapy, covering medical questions, home life, and emotional support.
Cooking For Chemotherapy (Chef Ryan) Specializes In Helping Cancer Fighters Overcome Many Eating-Related Chemotherapy Side-Effects.
Discover 68 Thoughtful And Comforting Gifts For Chemo Patients. From Practical To Pampering, Find The Perfect Way To Show Your Love And Support.
