Hormone therapy is a treatment option for cancers that grow using hormone signals, not all cancer types can benefit from this treatment option. Cancers with tumours that are hormone-sensitive are typically candidates for this treatment modality. Hormone therapy is typically a life-long treatment which can be difficult for patients to manage, therefore making an informed decision is critical.
Some cancers continue to grow because they can respond to hormone signals in the body. Those hormone signals act like instructions telling the cancer cells to keep growing. The goal of hormone therapy is to interrupt the delivery of these instructions and thus prevent the cancer cell from growing.
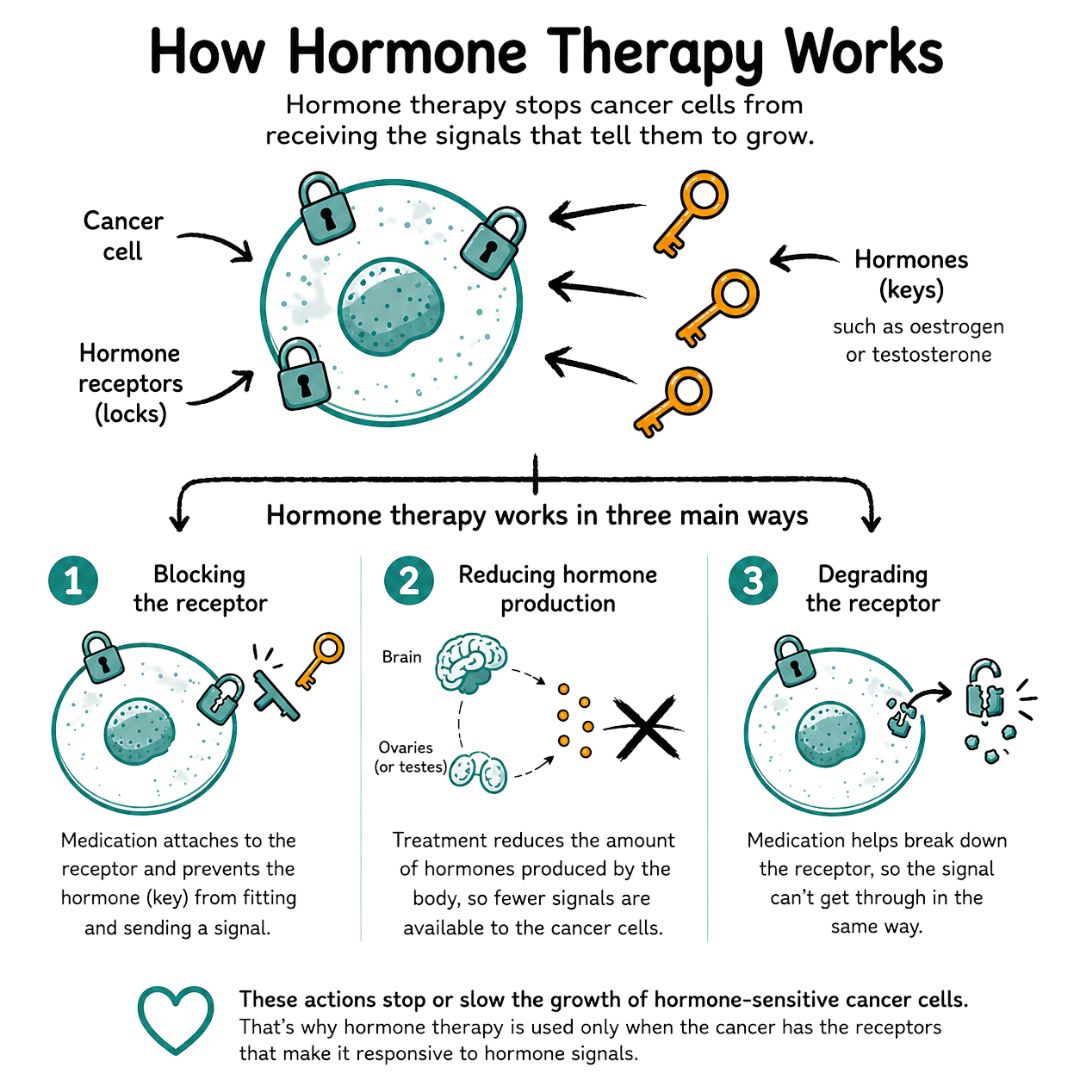
A simple way to understand this concept is to compare it to a lock and key. The lock is the receptor on or in the cancer cell. The key is the hormone, such as oestrogen or testosterone. When the right key fits the lock, the cell receives a signal to grow.
Hormone therapy helps by doing one of two things:
This is why hormone therapy is used only when the cancer is biologically hormone-sensitive. The American Cancer Society's explanation of hormone therapy describes this approach as blocking the receptor, degrading the receptor, or lowering the body's production of the hormone.
In order for hormone therapy to work, the tumour's biology is important. Hormone therapy will not work for cancers where the tumour growth is not dependent on hormone signals. It is possible for two people to have breast cancer, but only one benefits from hormone therapy. The factor that determines who will benefit is dependent on whether the cancer they have has the receptors that will make the tumour responsive to the hormone blocking treatment.
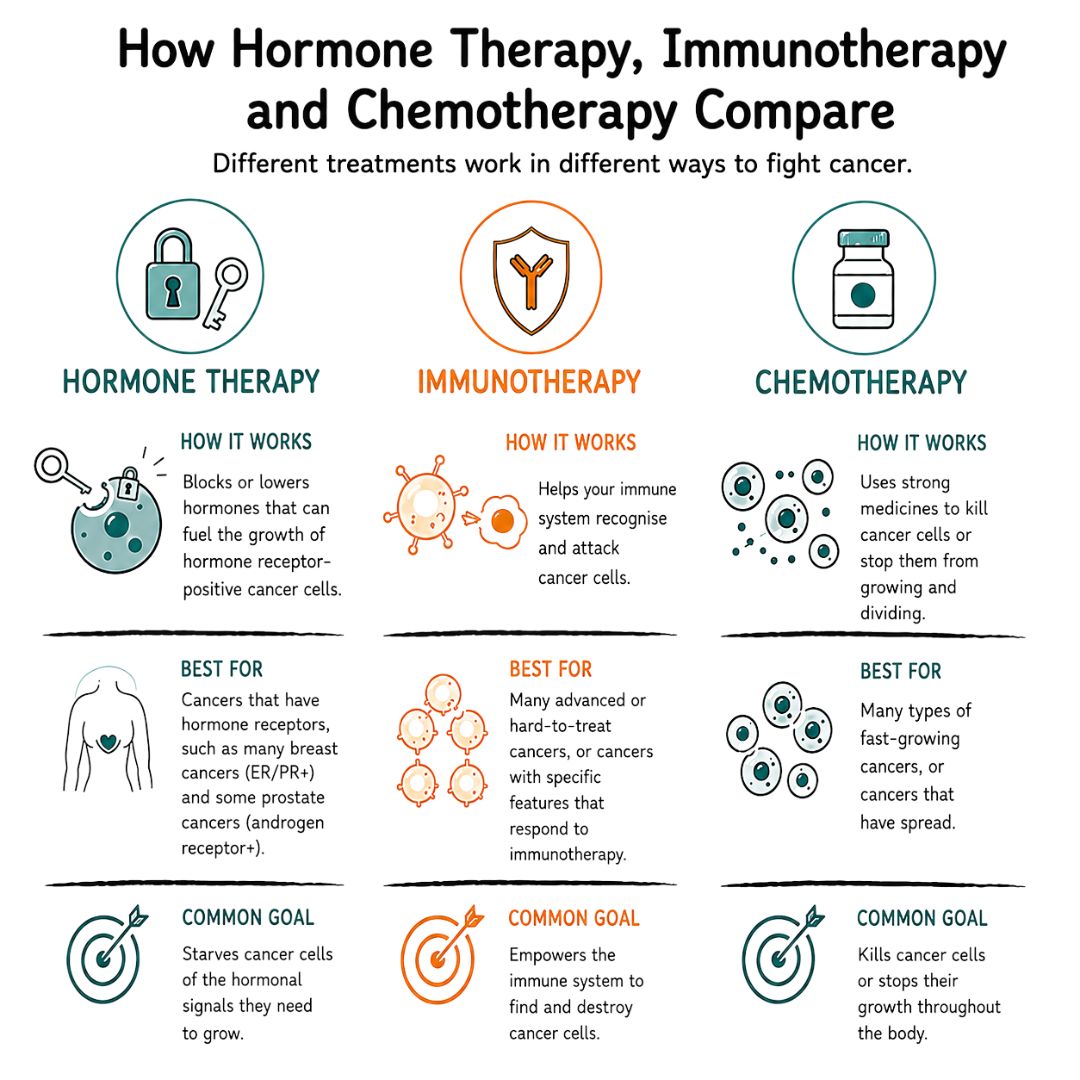
The deciding factor is whether the cancer has the receptors that make it responsive to hormone-blocking treatment. While some treatments like chemotherapy attack the cancer cells directly, hormone therapy works by disrupting the message that allows the cancer cells to keep growing.
The Hirschfeld Oncology's guide to hormone therapy can be a helpful resource to lean on to complement the medical advice you receive from the hospital.
Hormone therapy is one option amongst many for cancer treatment, and it can be confusing or overwhelming for patients to digest. Reading about other therapy options like immunotherapy can help distinguish one from another especially when multiple options are discussed.
The cancers most commonly treated with hormone therapy are breast cancer and prostate cancer. There are also situations where clinicians may consider hormone-based treatment in some other cancers, but in these cases the tumour has to be hormone-sensitive.
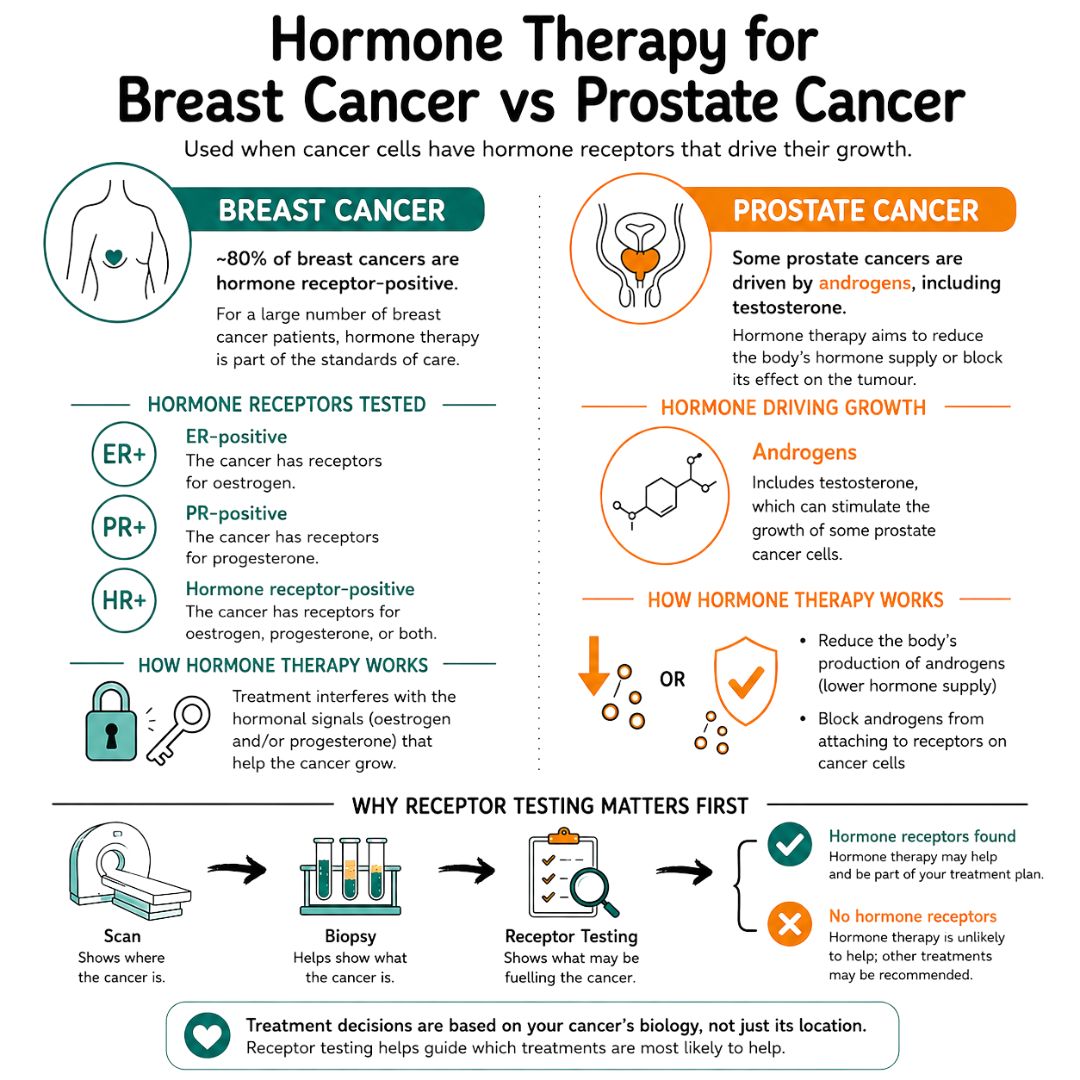
A scan can show where a cancer is. A biopsy helps show what the cancer is. Receptor testing adds another layer by showing what may be fuelling it.
That's why treatment decisions are rarely based on the cancer site alone. The pathology report often shapes whether hormone therapy is offered, which medicine is chosen, and whether it's likely to help enough to justify long-term use.
Hormone therapy is a major part of treatment for many breast cancers because roughly 80% of breast cancers are hormone receptor-positive, meaning the tumour cells have receptors for oestrogen, progesterone, or both, as outlined by Columbia Cancer. For a large number of breast cancer patients, hormone therapy is part of the standards of care.
A breast cancer may be described as:
If those receptors are there, treatment can be designed to interfere with the hormonal signals helping the cancer grow.
Prostate cancer is another common example because some prostate cancers are driven by androgens, including testosterone. In those cases, treatment may aim to reduce the body's hormone supply or block its effect on the tumour.
A more detailed overview is available in this guide to hormone therapy for prostate cancer, which can be useful when a family is trying to compare how hormone treatment works in different cancers.
Tamoxifen, aromatase inhibitor, ovarian suppression, injection, tablet are all terms that can be overwhelming for a patient that is first learning about hormone therapy.
The simplest way to make sense of it is to focus on what the treatment does and how it's given.
| Drug Class | Example | How It Works | How It's Given |
|---|---|---|---|
| Selective oestrogen receptor modulators | Tamoxifen | Blocks oestrogen from attaching to the receptor in breast tissue | Usually a tablet |
| Aromatase inhibitors | Anastrozole (Arimidex) | Lowers oestrogen production in the body | Usually a tablet |
| Selective oestrogen receptor degraders | imlunestrant (Inluriyo) | Helps degrade the receptor so hormone signalling is disrupted | Often an injection, though some settings may differ |
| Ovarian suppression treatment using gonadotropin-releasing hormone agonists | Leuprolide | Reduces hormone production from the ovaries | Commonly an injection |
| Hormone-lowering treatment for prostate cancer | Flutamide | Reduces or blocks hormone signals that can drive prostate cancer | Often an injection, sometimes with tablets depending on the medication |
The choice depends on several practical factors, not just the cancer name.
The specific treatment chosen requires an individualized approach to identify the best option for the patient depending on their age, stage of cancer and stage of life they are at.
Hormone therapy can be delivered in various ways including:
It is common for patients to want more information on how a long-term treatment like hormone therapy fits into the wider scope of their cancer diagnosis and stage of disease. This explanation of metastasis and breast cancer can help with that broader understanding.
Since hormone therapy changes or blocks the body's normal hormone signals, it can have a wide range of effects on the body as hormones play a major role in regulating and maintaining our body's balance.
The National Cancer Institute's hormone therapy overview notes side effects such as hot flushes, joint pain, mood changes, and bone loss, and these can make long-term adherence difficult. That matters because this treatment is often taken over years, not weeks.
Some symptoms are disruptive but manageable with support and small adjustments.
Side-effects of treatments can be challenging to manage and it is important to discuss these with your practitioner. Persistent symptoms should be reported, especially if they affect sleep, work, relationships, or the ability to keep taking treatment.
Hormones have a significant impact on mood and mental health. Introducing these intensive therapies can cause someone to become more anxious, flat, irritable, or tearful without realizing how much treatment is contributing. It is important to attend to your mental health needs just as much as your physical health. This guide to mental health support strategies may help patients and carers think about sustainable support.
For extra support around coping with overwhelm, this reVIBE Mental Health anxiety guide may be a useful companion to medical advice.
“How long will treatment last?” is often the question that lingers after everything else in the appointment has blurred together.
For early hormone receptor-positive breast cancer, treatment is often planned over a long stretch rather than a short course. In UK practice, guidance often supports treatment durations ranging from 5 to 10 years.
Hormone therapy is often used after the main treatment, such as surgery, to reduce the risk of the cancer returning. Given the benefit builds over time, the course may last years.
That can feel daunting. It's one thing to agree to treatment in principle. It's another to think about tablets, injections, check-ups, and side effects becoming part of ordinary life for a long period.
Some patients may struggle with the side-effects of hormone therapy options or may not be able to manage the treatment dosing. There are a variety of reasons a patient may want to discontinue hormone therapy. It is important to have these discussions with your healthcare providers in order to engage in shared-decision making about the best path forward.
If treatment feels unmanageable, the care team may discuss a different medication, a pause in the medications, strategies to manage the side effects and symptoms and review symptom trade-offs and overall benefits of the treatment.
Follow-up conversations about a patient's experience with hormone therapy should include whether the patient is missing doses, whether side effects are changing daily life, and whether the original plan still feels realistic.
Families often help here. They may notice that someone is moving less because of joint pain, sleeping badly, or becoming withdrawn. Those details can shape better decisions and more tolerable treatment.
When an oncology team recommends hormone therapy, they are choosing a treatment that fits the biology of the cancer. For the right cancer, that can be a very important part of treatment after surgery, before local treatment, or when cancer has spread and needs long-term control.
A doctor usually brings up hormone therapy after looking at tumour test results. In breast cancer care, for example, teams often test whether the cancer has receptors for oestrogen or progesterone. If those receptors are present, the cancer may respond to hormone treatment.
Cancer treatments are require an individualized approach. One person may be offered surgery and chemotherapy. Another may be offered surgery and hormone therapy. Another may need a combination. The difference often comes down to what the tumour is driven by.
A Consideration: If a doctor recommends hormone therapy, it's worth asking which hormone receptors were found and how that result changes the treatment plan.
It is important to ask questions during these consultations to ensure you have all the information needed to make an informed decision about the treatment option you would like to pursue. It often helps to bring a relative, take notes, or prepare questions in advance. A structured prompt list like these questions to ask an oncologist can make the next appointment feel more manageable.
Landmark UK-based evidence, including the Million Women Study discussion in this review, helped establish the complex relationship between hormones and cancer risk. That's one reason personalized conversations with a doctor matter so much. Hormone-related treatment decisions are rarely one-size-fits-all.
Reliable support usually comes from a mix of people and resources:
Edit Template
We strongly advise you to talk with a health care professional about specific medical conditions and treatments.
The information on our site is meant to be helpful and educational but is not a substitute for medical advice.
Melanoma Is Not Just a Disease of the Elderly or Fair-Skinned—It Can Affect Anyone. Learn the Facts, Debunk the Myths, and Understand the Real Risk Factors Based on UK Statistics.
A clear guide to lobular breast cancer. Learn about the subtle symptoms, diagnosis, personalized treatment plans, and essential support resources.
It’s probably one of the worst things for someone to be told: “You have cancer,”
