The first few days after a colon cancer diagnosis often feel blurry. One appointment leads to another. New words appear quickly. Someone says “prognosis”, and it can sound like they are trying to predict your whole future in a single breath.
But that's not what a colon cancer prognosis is.
I want to speak to you the way I would speak to a patient and family sitting across from me in the clinic. Calmly. Clearly. Without false reassurance, but without taking hope away either. Colon cancer and prognosis are closely linked, but prognosis is never just one number, and it is never the whole story of a person.
If you are newly diagnosed, waiting for test results, supporting someone you love, or trying to make sense of what the doctors have said, this guide is here to help you slow things down and understand what matters.
A common moment goes like this. You hear that the biopsy confirms colon cancer. Then the team says they need more information before they can talk properly about prognosis. Many people go home and search online straight away. They find survival tables, frightening stories, and medical terms that seem to raise more questions than they answer.
That reaction is completely understandable.
Prognosis means your doctor’s best medical estimate of how the cancer is likely to behave and how treatment may help. It is not a final verdict. It is more like a working picture built from evidence, then adjusted as more test results come in.
For one person, prognosis may mean, “This looks very treatable, and surgery is the main focus.” For another, it may mean, “We need a broader plan that includes chemotherapy and careful monitoring.” The same word can cover very different situations.
This is one reason families often feel confused. They expect one clear answer, but colon cancer care usually begins with several pieces of information arriving at different times. The colonoscopy confirms the diagnosis. Scans show where the cancer is. Pathology adds detail about the tumour itself. Blood tests and biomarker testing may refine the picture even more.
A prognosis is most useful when you ask, “What does this mean in my case?” rather than “What happens to everyone?”
If you have reached this article because you first noticed changes in your body and want to understand the bigger picture, it may help to read about possible colon cancer symptoms alongside this guide.
The most helpful way to approach colon cancer prognosis is to move one step at a time. First, understand what prognosis means. Then learn how doctors build it. Then ask what makes your situation unique.
Think of prognosis like a weather forecast. A forecast uses a lot of information. Wind patterns, pressure, temperature, and local conditions help meteorologists make the best prediction they can. But even an excellent forecast is still a prediction, not a promise.
Cancer prognosis works in a similar way.
Doctors use large amounts of past data, along with your scans, pathology, blood tests, and overall health, to estimate what is most likely. That estimate helps them recommend treatment. It does not lock your future into place.
A prognosis is not there to frighten you. It helps your team answer practical questions such as:
Without prognosis, treatment planning would be much less precise.
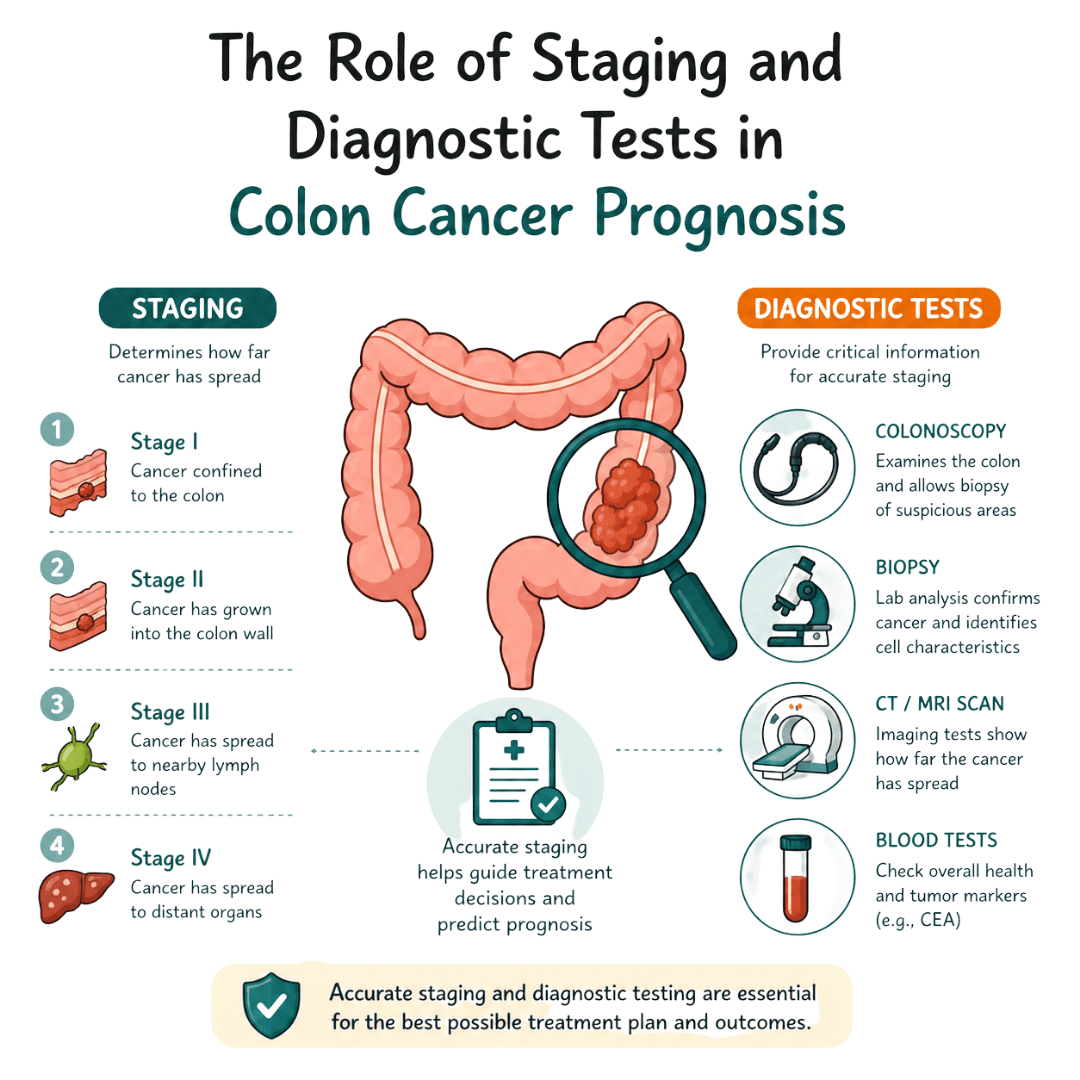
When clinicians discuss colon cancer prognosis, they usually draw on three broad areas.
First is the stage. This describes how far the cancer has grown or spread. Stage often has the biggest influence on prognosis.
Second is tumour biology. Two people can both have colon cancer, but their tumours may behave differently under the microscope or on biomarker testing. Features such as MSI or KRAS can matter because they may suggest a better fit for certain treatments.
Third is your overall health profile. A person’s strength, other medical conditions, recovery from surgery, and response to treatment all shape the practical outlook.
It does not mean that a doctor can tell exactly how long someone will live.
It does not mean every person with the same stage will have the same outcome.
It does not mean you should compare yourself too closely with a friend, neighbour, or story you read online. Even when the diagnosis sounds similar, the details are often very different.
Prognosis gives direction. It does not erase uncertainty, but it can turn uncertainty into a plan.
That plan may change over time. If a scan shows treatment is working well, the picture improves. If pathology reveals a tumour feature that responds to a certain drug, options may widen. If recovery is slower than expected, the team may adjust timing or priorities.
This is why many oncologists avoid reducing prognosis to one sentence. The fuller question is usually better: “Based on my stage, biology, and health, what does my outlook look like now, and what could change it?”
Once colon cancer is confirmed, the team starts gathering evidence. Each test answers a different question. One test confirms that cancer is present. Another shows location. Another helps estimate whether it has travelled. Another gives clues about how it might respond to treatment.
Many teams describe colon cancer using TNM.
A simple way to picture this is to think of a tree in a garden.
The T part asks how large the tree is and how far its roots have gone into the soil around it.
The N part asks whether nearby flowerbeds are affected.
The M part asks whether seeds have travelled to a different garden entirely.
Doctors then group TNM findings into stages. That stage helps shape treatment and prognosis.
A person usually meets these tests in sequence, although the exact order can vary.
This is often where the diagnosis begins. During the colonoscopy, the specialist sees the abnormal area directly and takes a biopsy. The biopsy tells the team whether the cells are cancerous.
This is the point where many patients first hear the phrase “we need staging scans”. That means the biopsy answered what it is, but not yet how much there is.
CT scans help doctors look beyond the colon itself. They are used to check whether there is any sign that the cancer has spread. Treatment for disease confined to the bowel is different from treatment for disease that has travelled elsewhere.
If you are trying to understand how advanced bowel cancer is discussed in patient-friendly language, this guide to stage 4 bowel cancer may help place some of those terms into context.
Blood tests give general information about your health, such as how your liver, kidneys, and blood counts are functioning. A blood marker called CEA may also be checked. It is not a stand-alone test for diagnosis, but it can be useful as part of monitoring over time.
Modern prognosis is not based only on where the cancer is. It also depends on what kind of cancer it is at a molecular level.
MSI and KRAS are two examples you may hear. These are not symptoms you feel. They are laboratory findings that can help the team understand tumour behaviour and treatment options.
According to information on MSI testing and expanded access to targeted immunotherapy, high MSI tumours are found in 20% of stage 2 cases, and NHS England’s 2025-2026 rollout of expanded MSI testing aims to improve prognosis for 5,000 more UK patients annually by improving access to targeted immunotherapy.
That kind of testing can change the conversation from “You have colon cancer” to “You have this specific subtype of colon cancer, and that affects the best treatment path.”
No single test tells the whole story. Together, they create the map your team uses.
Survival statistics are often the hardest part to read. They can also be the easiest part to misunderstand.
When doctors talk about survival rates, they are talking about groups of people treated in the past. They are not reading an individual future. That distinction matters a great deal.
A 5-year net survival rate tells us how many people are alive five years after diagnosis, after accounting for deaths from causes other than that cancer. It does not mean a person will only live for five years. Many people live much longer than that.
It also does not capture everything that is changing now. Treatments improve. Scans improve. Surgical techniques improve. Biomarker testing improves. So the figures are useful, but they are backward-looking by nature.
According to colon cancer survival statistics, the 5-year net survival rate is about 65%, up from 51% a decade prior. The same source reports 91% 5-year survival for localised disease, 74% for regional spread, and 16% for metastatic cancer.
| Stage | Description | Approximate 5-Year Net Survival Rate |
|---|---|---|
| Localised | Cancer is confined to the bowel | 91% |
| Regional | Cancer has spread to nearby tissues or lymph nodes | 74% |
| Metastatic | Cancer has spread to distant parts of the body | 16% |
| Overall | Across all stages combined | 65% |
These figures help explain why early diagnosis matters so much. They also show why stage is only the starting point in colon cancer and prognosis discussions.
People often read a table like this and mentally place themselves inside it. That is a very human reaction. But statistics do not know your exact pathology, your operation results, your biomarker profile, your general health, or how well your body responds to treatment.
A statistic also does not know whether your treatment team found the cancer after symptoms, after screening, or during work-up for something else. It does not know whether surgery removed all visible disease. It does not know whether newer treatment approaches may suit your tumour especially well.
Use survival figures as background information, not as a prediction written specifically for you.
If you want help making sense of how statistics are built and why averages do not always apply neatly to individuals, this article on cancer research and biostatistics can make that language easier to follow.
Try asking these questions instead of focusing only on the headline number:
Those questions bring the discussion back to the person who matters most. You.
Two people can both hear “colon cancer” and still have very different outlooks. That is because prognosis is built from layers. Stage matters, but it is not the only influence.
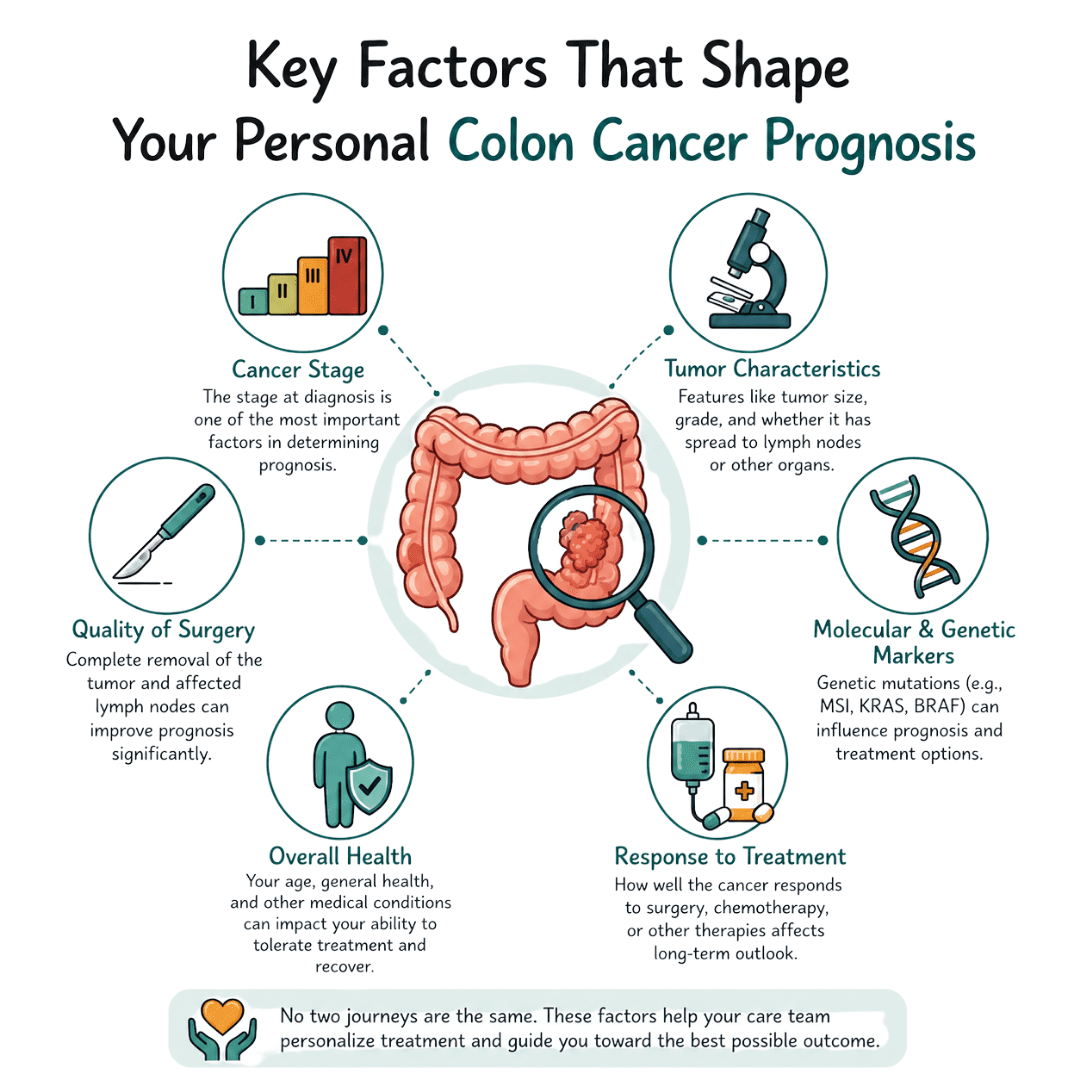
A surgeon may remove a tumour completely, yet the pathology report can still add important detail. Doctors look at how abnormal the cells appear, whether nearby lymph nodes contain cancer, and whether there are signs that tumour cells have entered blood vessels or lymph channels.
These details help explain risk more precisely. A stage label is a summary. The pathology report is the fine print.
Some cancers also carry inherited or molecular patterns that change how doctors think about prognosis and treatment. If your team mentions family history or genetic risk, learning about Lynch syndrome related cancers can help you understand why those questions matter.
Doctors do not treat a scan. They treat a person.
Someone who is otherwise well may recover from surgery more smoothly and be more able to receive further treatment on time if needed. Another person may be coping with heart disease, diabetes, frailty, or other medical issues that make treatment planning more delicate.
This does not mean “fit” patients deserve better outcomes. It means prognosis is always tied to what treatments are safe, realistic, and tolerable for the whole person.
The first version of a prognosis is not always the final one.
A cancer that responds well to treatment may shift the conversation in a more hopeful direction. A recovery that is slower or more complicated may mean timelines need adjusting. Follow-up scans, blood tests, and clinic reviews often refine the outlook over time.
For some people, the most accurate prognosis is the one discussed after surgery, when the team can combine the scan results with the full pathology findings.
This part is often left out of patient guides, but it matters.
Where a person lives, how easily they can reach appointments, whether they can take time off work, and how quickly they can access investigations can all shape outcomes. In England, colorectal cancer outcomes differ by deprivation level. People in the most deprived areas have a 45% higher colorectal cancer mortality rate, and their 5-year net survival is 52% compared with 64% for people in the least deprived areas.
That does not mean an individual’s future is determined by postcode or income. It does mean prognosis is not purely biological. Access, timing, support, and health system navigation matter.
If getting to appointments, understanding paperwork, or arranging help at home is difficult, tell your team early. Practical barriers can affect care, and teams can often help more when they know sooner.
Try grouping your questions into four areas:
When those four areas are discussed together, prognosis becomes more realistic and more personal. It stops being a scary abstract term and becomes a plan built around your actual life.
Good prognosis conversations rarely happen by accident. They happen when patients and families know what to ask, and when they give themselves permission to ask it more than once.
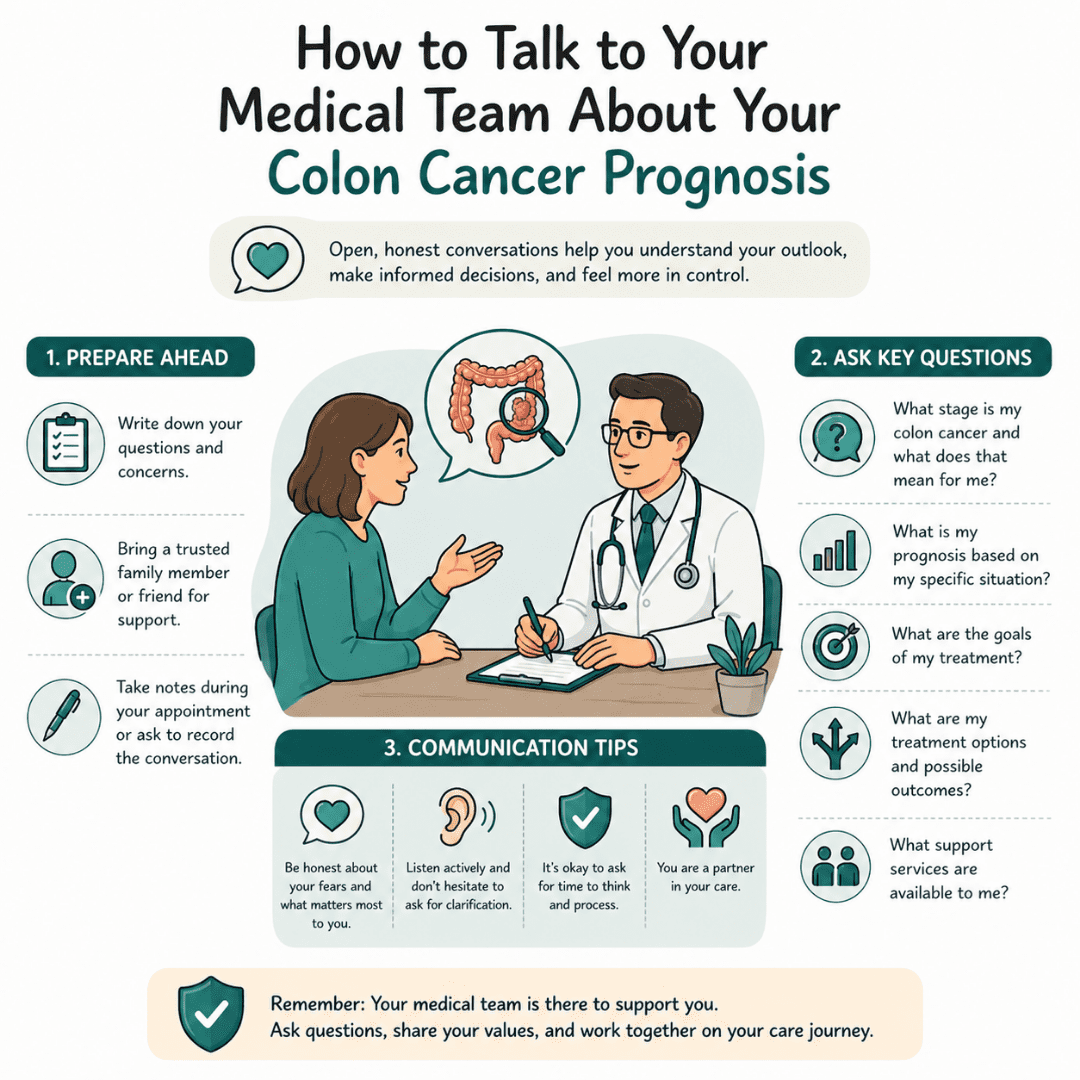
A clinic appointment can move quickly. It helps to bring a notebook, take someone with you if possible, and write your questions in advance. If you become overwhelmed halfway through, that is normal. Ask the doctor or specialist nurse to pause and repeat things in simpler language.
You do not need to ask all of these at once. Choose the ones that fit where you are now.
For stage 3 colon cancer, Cancer Research UK bowel cancer survival information notes that adjuvant chemotherapy after surgery improves disease-free survival by 20-30%. The same source says discussing NICE guidelines (NG151) on biomarker testing and surveillance with your multidisciplinary team is important, and that each 4-week delay in starting adjuvant therapy can worsen overall survival by 6-10%.
That is one reason timing questions are not “fussy” questions. They are part of good care.
Some people worry about seeming difficult. In reality, clear questions usually help clinicians care for you better.
You can try phrases like:
If speaking up is hard for you, this guide on how to advocate for yourself with your healthcare provider offers practical ways to prepare for appointments and communicate your needs clearly.
A short video can also help you think about how these conversations unfold in real life:
It is honest. It is specific. It leaves room for uncertainty without being vague.
You should come away understanding the current picture, the treatment plan, what may change the outlook, and when you will get more information. If that did not happen, it is reasonable to ask for another conversation.
You are not asking for “too much” when you ask for clarity. Understanding your prognosis is part of your care.
Even when information is delivered kindly, prognosis can land heavily. Some people want every detail straight away. Others need smaller pieces over time. Both responses are normal.
Fear and hope often sit side by side. You may feel relieved to have a plan and frightened by the same conversation. Family members may cope differently from one another, which can create tension even when everyone means well.
Try to notice what kind of support you need right now.
If a stoma or bowel diversion is part of your treatment, reading about what a colostomy is can make those discussions less daunting.
It is sensible to think about work, childcare, transport, finances, and who can come to appointments. Good planning reduces stress and gives you more control.
The importance of timely diagnosis is clear in the UK data. According to SEER stat facts referenced in the verified data provided, the 5-year net survival is 91.3% for localised colon cancer and 16.9% for distant metastasis, which is one reason screening and early investigation matter so much.
For life during treatment, practical support matters too. Cancer Care Parcel offers guides, webinars, and supportive resources for people affected by cancer. If you need comfort items or patient-friendly education alongside medical care, it is worth exploring their wider support options.
Living with a prognosis means living with some uncertainty. That is hard. But many patients feel steadier when uncertainty is paired with a clear next step, a support network, and reliable information.
Some questions do not fit neatly into a long discussion with the oncologist. A quick reference can help.
| Question | Answer |
|---|---|
| Can my prognosis change after treatment starts? | Yes. Doctors often refine prognosis after surgery, pathology review, and early response to treatment. |
| Does a 5-year survival rate mean I only have 5 years to live? | No. It is a statistical benchmark used to track outcomes in groups of patients. Many people live well beyond that point. |
| Should I read survival statistics online? | You can, but read them carefully. They describe groups, not individuals, and older data may not reflect newer treatments. |
| What if I do not want exact numbers? | Tell your team. You can ask for the “big picture” without hearing detailed percentages. |
| When should palliative care be discussed? | Palliative care is not only for the last days of life. It can be introduced alongside active treatment to help with symptoms, decision-making, and support. For a simple overview, this guide to palliative and end-of-life care may help. |
| What matters most in a prognosis conversation? | Understanding what is known, what is still uncertain, what the treatment plan is, and what your next step should be. |
We strongly advise you to talk with a health care professional about specific medical conditions and treatments.
The information on our site is meant to be helpful and educational but is not a substitute for medical advice.
The Thoughts Of Cancer Returning Still Seep Back In My Brain Upon Occasion, But I Quickly Replace Them With Gratitude That I Am Still Here
Maintaining A Positive Attitude And Having Strong Faith Made A Significant Impact On My Ability To Overcome Adversity.
Facing a stage 4 bowel cancer diagnosis? This clear guide explains what it means, how it spreads, treatment options, managing symptoms, and ways to protect your quality of life, empowering you with facts and next steps.
