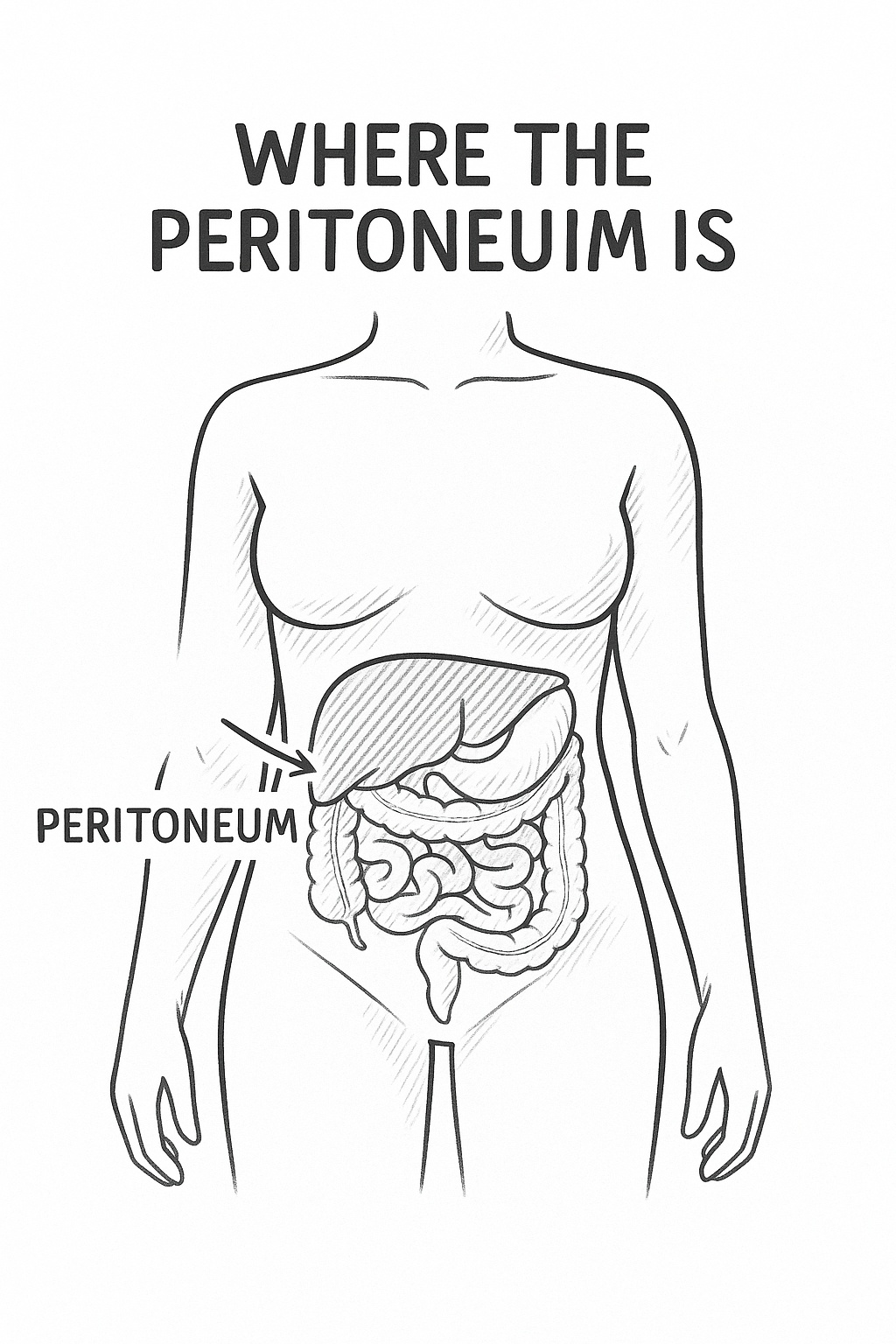
Primary peritoneal cancer, often called PPC, is a rare cancer that begins in the peritoneum. This is the very thin, delicate layer of tissue that lines the inside of your abdomen and covers most of your abdominal organs.
A good way to picture it is to think of the inside of your abdomen as a room. The peritoneum would be the wallpaper, covering the inner walls and wrapping around all the furniture—your stomach, liver, and intestines. It's not just a passive lining; it produces a lubricating fluid that allows your organs to move smoothly against each other.
Unlike other cancers that might spread to the peritoneum from somewhere else, PPC starts right there, on the 'wallpaper' itself.
The "primary" part of the name is crucial. It means the cancer originated in the peritoneum. This is different from what are known as peritoneal metastases, which is when cancer cells from another organ—like the bowel or stomach—travel and set up a new tumour in the peritoneum. You can learn more about how cancer can spread in our detailed guide on metastatic cancer.
PPC is genuinely rare. To put it into perspective, the age-adjusted incidence rate is around 6.78 per million people. This is a tiny fraction compared to ovarian cancer, which has a rate of 119.9 per million. It’s clear from these figures just how uncommon PPC is among gynaecological cancers. For a deeper dive into these numbers, you can read the full research on incidence rates.
One of the most important things to grasp about PPC is how closely it resembles the most common type of ovarian cancer, known as epithelial ovarian cancer. The reason for this is fascinating—it goes all the way back to how we develop as embryos. The tissue that forms the peritoneum and the tissue that covers the surface of the ovaries actually come from the same cell layer.
Because of this shared heritage, the two cancers look and act like close relatives.
This striking similarity is why primary peritoneal cancer is almost always managed by a gynaecological oncology team—the very same specialists who treat ovarian cancer. It also explains why someone who has had their ovaries removed can still, unfortunately, develop PPC, as the peritoneal lining remains throughout the abdomen.
Keeping this fundamental link in mind is key. It helps make sense of why your diagnosis and treatment plan might look so similar to someone's with ovarian cancer, and it sets the stage for understanding the more specific details we'll cover next.
When you receive a diagnosis like primary peritoneal cancer, one of the first questions that often comes to mind is, "Why me?" It's a completely natural reaction. While we don't always have a straightforward answer for what causes this cancer, we do understand some of the factors that can increase a person's risk.
It's so important to remember this: having one or more risk factors doesn't mean you're destined to get cancer. In fact, many people diagnosed with primary peritoneal cancer have no obvious risk factors at all. Cancer is complex, and there’s absolutely no room for self-blame.
Our genes can play a major part in our risk profile. Think of your genes as an instruction manual for your body; sometimes, there are tiny "spelling mistakes" or mutations in those instructions that can be passed down through families.
If you have a strong family history of breast, ovarian, or peritoneal cancers, your doctor might recommend genetic counselling. It’s a helpful process where you can talk through your family history, understand your personal risk, and decide if genetic testing is the right step for you.
Genetics isn't the whole story. A few other factors can also influence a person's likelihood of developing this cancer.
Age is one of the biggest. The risk for primary peritoneal cancer tends to go up as we get older, and most women are diagnosed after menopause. This is a pattern it shares with its close cousin, ovarian cancer. A strong family history, even if no specific gene mutation has been found, is also considered a significant risk factor.
It is important to know that for many individuals, a specific cause is never identified. The development of cancer is a complex process, and sometimes it occurs without any identifiable genetic predisposition or lifestyle influence.
While certain cancers have clear links to lifestyle or environmental exposures, the connection isn't as well-defined for primary peritoneal cancer. That said, focusing on your overall well-being is always a good idea. Looking after yourself through positive lifestyle behaviours can support your health through any challenge, and your medical team can guide you on what’s best and safest for you.
The early signs of primary peritoneal cancer can be frustratingly vague. They often masquerade as everyday digestive troubles, making them all too easy to brush aside. But learning to recognise these signals is the crucial first step toward getting the medical attention you need.
Think of these symptoms as a quiet, persistent alarm from your body. The real clue isn't just a single day of feeling bloated; it's the persistence. We're talking about changes that don't go away, don't seem to get better, or even slowly start to feel worse over time.
It makes sense that most of the common signs of primary peritoneal cancer are felt in the abdomen, as the peritoneum is the very lining of that space. This is why paying close attention to new and lasting changes in this area is so important.
The most common symptoms people report include:
As the cancer develops, other, more general signs can appear too. You might notice unexplained weight loss, a deep fatigue that sleep doesn't fix, nausea, or a general loss of appetite. It's really the combination of these symptoms, and the fact that they stick around, that should prompt a chat with your doctor.
It can be hard to tell what's a minor issue and what might be more serious. The table below helps outline some of the differences.
| Symptom | Possible Benign Cause | When It Could Indicate PPC (Seek Medical Advice) |
|---|---|---|
| Bloating | Trapped wind, food intolerance, menstrual cycle. | The bloating is constant, doesn't ease overnight, and is accompanied by other symptoms like pain or feeling full quickly. |
| Abdominal Pain | Indigestion, muscle strain, irritable bowel syndrome (IBS). | The pain is a persistent, dull ache or pressure that is new for you and doesn't resolve within a week or two. |
| Feeling Full Quickly | Eating rich foods, stress, or eating too fast. | This happens with almost every meal, even small ones, and you may also be losing weight without trying. |
| Bowel/Bladder Changes | Dehydration, dietary changes, minor infection. | The changes (e.g., new constipation, increased urgency) last for more than a few weeks and become your 'new normal'. |
Ultimately, a single symptom on its own may not be a cause for alarm, but a cluster of persistent symptoms definitely warrants a visit to your doctor.
Trust your gut, literally. You are the expert on your own body, and you know what feels normal for you. When something feels consistently "off," it deserves to be looked into. Too often, these subtle symptoms get chalked up to ageing, menopause, or IBS, which can lead to delays in getting a diagnosis.
It is so important not to dismiss persistent and unusual changes in your body. While these symptoms can be caused by many non-serious things, ruling out something like primary peritoneal cancer early gives you the very best chance for effective treatment.
Being a good advocate for your health means going to your doctor's appointment prepared. Try keeping a simple diary of your symptoms: note what they are, how often they happen, and how they're affecting your day-to-day life. This kind of specific information gives your doctor a much clearer picture of what's going on. For more practical advice on these conversations, take a look at our guide on how to make yourself heard by medical professionals. When it comes to your health, getting checked out early is always the right move.
Hearing the words "it could be cancer" is often the start of an overwhelming and anxious journey. When it comes to primary peritoneal cancer, figuring out what's really going on can be a confusing process. Understanding the steps involved can give you a clearer roadmap of what to expect, helping you feel more in control and ready to ask the right questions.
The journey usually starts with a trip to your doctor, likely because of persistent symptoms like bloating, stomach discomfort, or feeling full too quickly. From there, your doctor will start a series of tests to get a better look at what’s happening inside your body.
The first stage is all about gathering clues, usually with tests that aren't too invasive. The goal is to see if there are any signs pointing towards a gynaecological cancer, which helps your medical team decide what to do next.
One of the first things they'll likely do is a blood test to check for a tumour marker called CA-125. This is a protein that can be higher than normal in people with primary peritoneal cancer. It’s a useful indicator, but it’s not a standalone diagnostic tool—plenty of other, non-cancerous conditions can also cause CA-125 levels to rise.
At the same time, you’ll probably be sent for imaging scans to create detailed pictures of your abdomen and pelvis.
Think of these initial steps like a detective gathering evidence. Each result provides another piece of the puzzle. The image below shows how these seemingly common symptoms are often the starting point for this vital investigation.
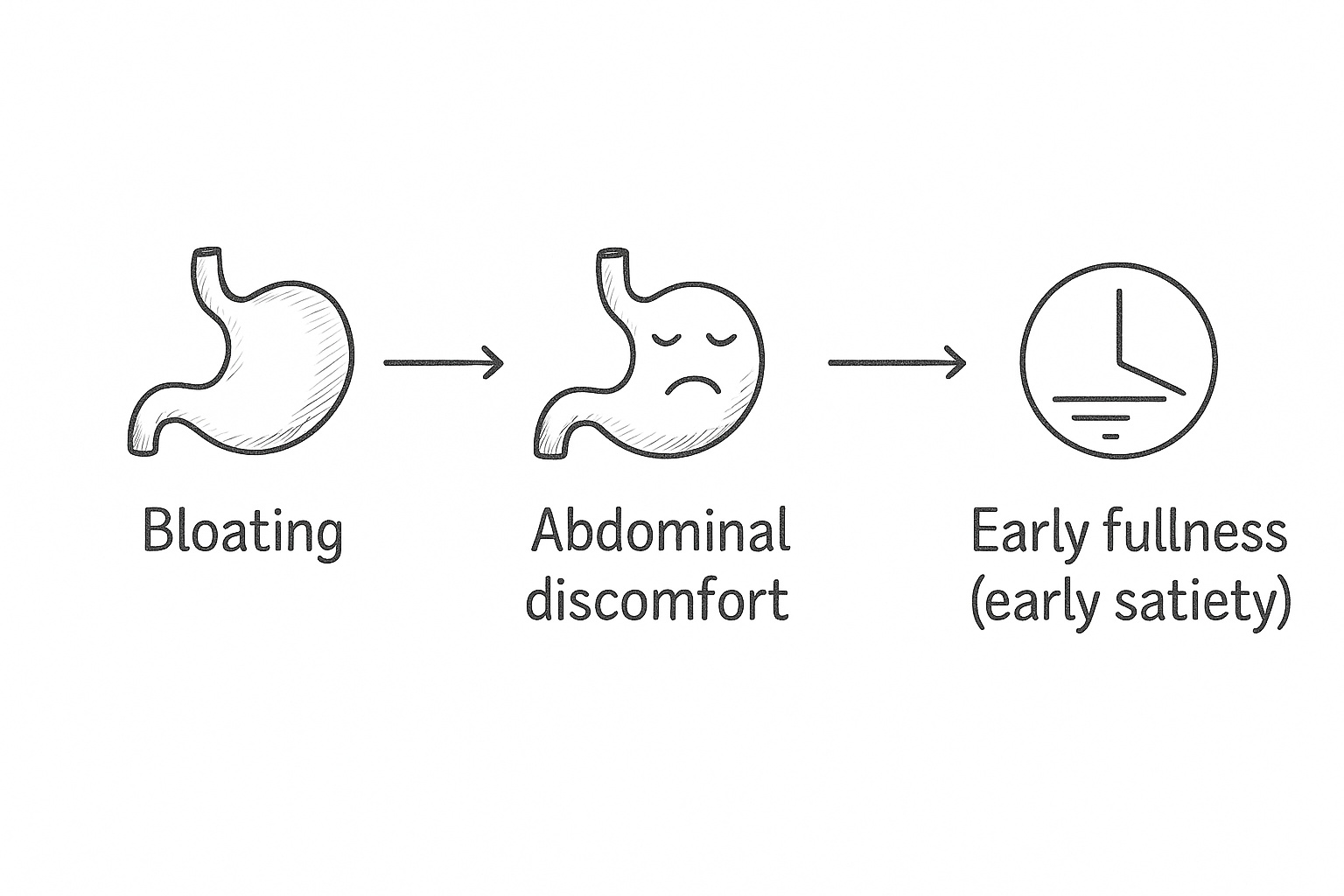
This really brings home how persistent issues like bloating, discomfort, and feeling full are key signals that need to be checked out by a doctor.
While blood tests and scans can point strongly in one direction, the only way to be 100% certain it's cancer is with a biopsy. This is where a specialist takes a tiny sample of tissue from the suspicious area to be examined under a microscope.
For suspected primary peritoneal cancer, this is often done during a minor 'keyhole' surgery called a laparoscopy. A surgeon makes a small cut in the abdomen and inserts a thin tube with a camera on the end. This allows them to see the peritoneum directly, assess the situation, and take the tissue samples needed for a definitive answer.
A biopsy is the gold standard for diagnosis. It doesn't just confirm if cancer is present; it also reveals the specific type of cancer cell, which is crucial for figuring out the most effective treatment plan.
Once the diagnosis is confirmed, the next vital step is staging. This is the process of working out the extent of the cancer—how much there is and if, or where, it has spread. Unfortunately, because the symptoms of primary peritoneal cancer can be so vague, it’s often diagnosed at a more advanced stage.
Research shows that the vast majority of people are diagnosed when the disease is at stage III or IV—somewhere around 77% to 78% of all cases. You can read more about the research on cancer staging data at cancer.gov.
Staging is incredibly important because it guides your entire treatment plan. Your oncology team will use all of this information to build a strategy that's tailored specifically for you. Knowing what to expect can make a real difference, and you can find more practical advice in our article on how to improve your cancer diagnosis experience.
When you’re first diagnosed with primary peritoneal cancer, understanding the treatment options can feel overwhelming. Your medical team will walk you through a plan they’ve tailored specifically to you, considering the cancer’s stage, your overall health, and your personal circumstances.
The approach is usually a powerful combination of treatments. Think of it as a coordinated attack: surgery takes aim at the bulk of the cancer, while other therapies are sent in to track down and eliminate any cells left behind. This is a highly specialised field, and your care will typically be led by a gynaecological oncology team with deep experience in this exact type of cancer.
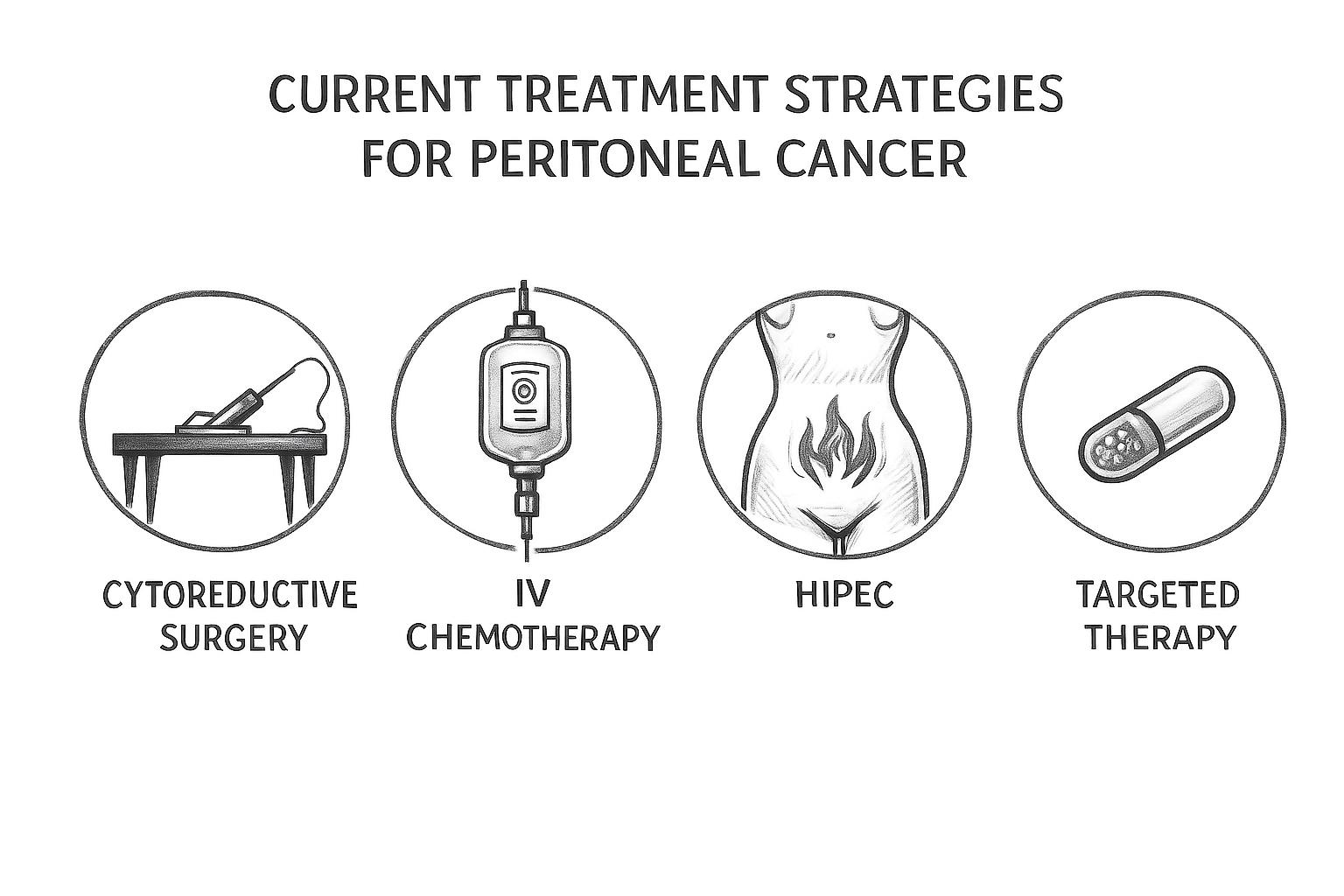
Let's break down the main strategies you’ll likely discuss with them.
Surgery is the cornerstone of treating primary peritoneal cancer. The main operation is called cytoreductive surgery, but you’ll often hear it called "debulking." The goal is just as it sounds: to reduce the amount of cancer in the body as much as humanly possible.
During the procedure, the surgeon will painstakingly remove every visible trace of the tumour from the peritoneum and any organs it has touched. Success is measured by achieving 'optimal debulking', which means no visible cancer spots larger than 1cm are left. The ideal outcome, of course, is no visible disease at all. The less cancer that remains, the more effective the follow-up chemotherapy can be.
This can be a very extensive operation. It might involve removing the ovaries, fallopian tubes, uterus, and even parts of other organs. It's a major undertaking, but it's one of the most critical steps in getting the disease under control.
Chemotherapy uses powerful drugs to destroy cancer cells or halt their growth. It's an absolutely vital part of the treatment plan for primary peritoneal cancer and can be delivered in a couple of different ways.
Intravenous (IV) Chemotherapy
This is the most common method. Chemotherapy drugs are administered through a drip directly into a vein, allowing them to travel throughout your bloodstream. Because it reaches almost every part of the body, it’s known as a systemic treatment.
Intraperitoneal (IP) Chemotherapy
Sometimes, a more direct approach is better. IP chemotherapy delivers the drugs straight into the abdominal cavity via a small, soft tube. This essentially 'bathes' the peritoneum in a highly concentrated dose of the cancer-fighting medicine, putting it right where it's needed most.
A very specialised form of this is HIPEC (Hyperthermic Intraperitoneal Chemotherapy).
In recent years, treatments have become much smarter. Unlike traditional chemotherapy, which affects all rapidly dividing cells (both cancerous and healthy), targeted therapies are designed to zero in on specific weaknesses in the cancer cells themselves.
For primary peritoneal cancer, two main types have proven valuable:
These advanced medicines are pushing cancer care towards a far more personalised future. To get a better sense of how genetics is shaping these new approaches, have a look at our article on decoding DNA as a tool for personalised chemotherapy.
Medical progress doesn't happen by accident; it’s driven by research. Clinical trials are studies that test new treatments and innovative ways of using existing ones. For someone with a rarer cancer like this, joining a trial can provide access to promising new therapies that aren't yet standard practice.
Don’t hesitate to ask your oncology team if there are any clinical trials that might be right for you. It’s a very personal choice, but it can be an empowering way to play a role in advancing science while potentially gaining access to the very latest in cancer treatment.
Finishing active treatment for primary peritoneal cancer is a major milestone, but it's also the start of a new chapter. This next phase is all about staying on top of your health, managing your long-term well-being, and knowing what to expect.
It’s completely normal to want to know about prognosis and survival rates. But it's crucial to understand that these numbers are just averages taken from very large groups of people. They can't tell your individual story or predict how you'll respond to treatment. The best person to talk to about your personal outlook is always a member of your medical team.
Once your main treatment ends, you’ll move into a period of regular follow-up care. This is an essential partnership between you and your oncology team, designed to monitor your health closely and catch any potential issues as early as possible.
Your follow-up schedule will be tailored to you, but it usually involves a series of appointments that might include:
You can expect these appointments to be more frequent right after treatment, then gradually spread out over time as long as you remain well. This ongoing contact is as much for your peace of mind as it is for your physical health.
You’ll likely hear your care team use the terms remission and recurrence. Remission is the goal of all treatment—it means that tests and scans show no signs of cancer in your body.
Recurrence, however, is the term for when the cancer returns after a period of remission. Because this is a possibility with primary peritoneal cancer, your team will monitor you very carefully for any signs of it. Living with this possibility can bring its own set of emotional challenges, from ‘scanxiety’ before an appointment to a general sense of uncertainty.
Managing the emotional side of survivorship is just as important as the physical. Openly discussing your fears with your care team, a counsellor, or a support group can make a significant difference in how you cope with the journey ahead.
Survival outcomes for primary peritoneal cancer have historically been impacted by its tendency to be diagnosed at a later stage. Often, five-year survival rates have been lower than for ovarian cancer, partly due to the aggressive nature of the disease.
Living with a diagnosis like primary peritoneal cancer isn’t just about the medical side of things; it’s about prioritising your quality of life every single day. This means being proactive about managing any lingering treatment side effects and flagging any new symptoms as soon as they appear.
Palliative care is a huge part of this. It’s a common misconception that palliative care is only for the end of life. In reality, it’s a specialist type of medical support focused on providing relief from the symptoms, pain, and stress of a serious illness. The goal is simple: to improve quality of life for both you and your family.
Giving yourself the tools to understand your health is also incredibly powerful. You can explore effective patient education resources to feel more in control. This kind of holistic approach ensures that your comfort and well-being are always at the very centre of your care plan.
It's completely normal to have a lot of questions after a diagnosis of primary peritoneal cancer (PPC). To help, we’ve put together some straightforward answers to the questions we hear most often, giving you the key information you need in one place.
This is a really common question, and the answer is: they are very similar, but not exactly the same. Primary peritoneal cancer (PPC) begins in the tissue lining your abdomen (the peritoneum), whereas ovarian cancer starts in the ovaries themselves.
However, the cells in the peritoneum and on the surface of the ovaries are almost identical. This means both cancers behave in very similar ways, share the same symptoms, and have common risk factors, like the BRCA gene mutations. For this reason, treatments are the same, and your care will be handled by the same specialist team that looks after people with ovarian cancer. Think of them as very close cousins.
The main aim of treatment is to achieve a long-term remission, which for many people feels like a cure. The chances of this really depend on individual factors, like how advanced the cancer is when it's found and how well it responds to the first round of surgery and chemotherapy.
Because PPC is often diagnosed at a later stage, the focus of treatment can sometimes shift to controlling the disease for as long as possible while maintaining a great quality of life. It’s becoming more common for people to live for many years with PPC, managing it much like a chronic illness with treatments that keep it in check.
It's so important to remember that you are not a statistic. Survival rates are just averages from large groups of people and can't predict your individual outcome. Your medical team knows you and your situation best, so they are the ones to talk to about what your treatment journey might look like.
HIPEC is short for Hyperthermic Intraperitoneal Chemotherapy. It’s a very specialised treatment where a concentrated, heated dose of chemotherapy is washed directly through the abdomen at the end of surgery. The heat is a key part of it, as it helps the chemotherapy drugs penetrate more deeply and kill off any remaining cancer cells more effectively.
This is a major procedure and isn't suitable for everyone. It's only offered in a few specialist centres. Whether it's an option for you depends on things like your general health, how much the cancer has spread, and other medical considerations. It’s a complex decision that you would need to discuss in detail with your oncology team to carefully weigh up the potential benefits and the risks.
Getting a PPC diagnosis is a huge emotional blow, and it’s vital to build a strong support network to help you through it. Please remember, you don't have to face this on your own.
A great first step is to speak with your medical team. They are connected to a whole host of support services, including counsellors and psychologists who specialise in helping people with cancer. Many people also find enormous strength and comfort in speaking to others who are going through something similar.
Putting together this network of support is just as important as your medical treatment. A combination of professional help, the love of friends and family, and the understanding of peers can make all the difference.
We strongly advise you to talk with a health care professional about specific medical conditions and treatments.
The information on our site is meant to be helpful and educational but is not a substitute for medical advice.
Compassionate Emotional Healing Tips To Bring Comfort, Strength, And Understanding During The Cancer Journey.
I Am A 2x AML Leukemia Survivor And A Stem Cell Transplant Recipient And I Can Tell You It’s Not Whether Or Not You Fall, Its Whether Or Not You Get Back Up.
Yes! Men Get Breast Cancer Too. Discussing Breast Cancer Gift Ideas For All Breast Cancer Patients. Covering All Stages And Treatments.
