
Subtotal: £19.50

Subtotal: £19.50
Subtotal: £19.50
The consultant has just said the word stoma, and everything after that has gone a bit blurry.
You may have heard only fragments. A bag. An opening on the abdomen. Maybe temporary. Maybe permanent. Your partner might be trying to stay calm while wondering what daily life will look like. You might be thinking less about anatomy and more about ordinary things. Will I still sleep properly? Eat normally? Go out? Work? Feel like myself?
Those questions are sensible. They’re often the first ones people ask, even if they don’t say them out loud in clinic.
A colostomy or ileostomy is a change in how waste leaves your body. It can feel very personal, but it isn’t a failure and it isn’t the end of a full life. For many people having cancer surgery, a stoma is part of making treatment safer, relieving symptoms, or giving the bowel time to heal. The early period can be steep, but it usually becomes much more manageable once the shock settles and routines start to form.
Families often need support too. If the people around you are struggling to know how to help, practical guidance on strengthening your personal support network can make the whole experience feel less lonely and less chaotic.
People often arrive at this point feeling they have no language for what’s happening. One minute the focus is the tumour. The next, the conversation is about bowel diversion, stoma sites, pouching systems, and whether the change may be reversible later.
That jump can feel abrupt. It also makes many patients assume life will now be dominated by the stoma.
In practice, the first challenge is usually uncertainty, not the stoma itself. Individuals often don’t know the difference between colostomy vs ileostomy, and because the words sound technical, they can seem more frightening than they are. Once the terms are unpacked in plain language, the picture usually becomes clearer.
A stoma changes the route. It doesn’t erase the person you were before surgery.
The most helpful starting point is this. A surgeon isn’t choosing between two random procedures. They’re deciding which part of the bowel is safest and most useful to bring to the surface, based on where the cancer is, what operation you need, and whether the bowel needs protection while it heals.
For some people, a stoma is temporary and part of a treatment plan aimed at recovery. For others, it’s permanent and becomes part of long-term life after cancer surgery. Both situations carry emotional weight. Both can still include independence, intimacy, travel, meals out, exercise, and ordinary routine.
An ostomy is a surgically created opening on the abdomen that allows waste to leave the body through a stoma instead of passing through the rectum in the usual way. The waste is collected in a pouch attached to the skin.
When people compare colostomy vs ileostomy, the key difference is which part of the bowel forms the stoma.
A colostomy uses part of the colon, which is the large bowel. Because the colon normally absorbs water, the output is usually thicker or more formed.
An ileostomy uses the ileum, which is the lower end of the small bowel. Because this bypasses the colon, the output is usually looser and more liquid.
That one difference explains many of the daily life changes people notice later. It affects pouch choice, emptying frequency, skin care, hydration, and how cautious someone may need to be with certain foods.
If you'd like a simple primer focused just on the basics, this guide on what a colostomy is is a useful starting point.
In cancer care, surgeons may recommend a stoma for several reasons:
These words can sound intimidating, but they describe structure and purpose.
A temporary stoma is one that may be reversed later if the bowel heals well and your overall health allows another operation. A permanent stoma is intended to stay long term because reconnection isn’t possible or wouldn’t be safe.
A loop stoma is often created by bringing a loop of bowel to the surface. This is commonly used when diversion is needed for a period of healing. An end stoma is formed from the cut end of the bowel and may be used when a section has been removed and the bowel isn’t being rejoined at that time.
Useful question for clinic: “Is this stoma being created to protect healing, to relieve symptoms, or because reconnection won’t be possible?”
That question often gets you a clearer answer than asking only whether it is “temporary or permanent”.
The operations share a common idea, but recovery can feel different depending on which bowel segment is used, what cancer surgery was done alongside it, and whether the stoma is protecting a new join.
In many cases, an ileostomy is placed on the right side of the abdomen because it comes from the small bowel. A colostomy is often placed on the left side because it comes from the large bowel. There are exceptions, especially if the surgeon needs to work around scars, body shape, tumour location, or previous surgery.
Before surgery, a stoma care nurse will often mark the most practical spot on your abdomen. That small step matters. A good site can make clothing, movement, sitting, and pouch adhesion much easier afterwards.
Individuals often wake from surgery with a pouch already in place and a lot of questions. At first, even looking at the stoma can feel difficult. That reaction is common.
In hospital, your nursing team usually helps with the first essentials:
A common worry is, “What if I can’t do this myself?” Early on, many people can’t. Then they learn. Most need repetition, hands-on practice, and reassurance more than they need perfect confidence on day one.
One study of postoperative outcomes reported that ileostomies showed anastomotic healing rates of 80% at 1 week compared with 52% for colostomies, with better overall quality of life scores in that setting. The same report noted shorter operative time and less blood loss for ileostomy surgery, at 113 minutes versus 129 minutes and 8 g versus 40 g respectively, according to postoperative outcomes comparing ileostomy and colostomy.
That doesn’t mean ileostomy is always “better”. It means the surgical advantages in some settings have to be balanced against the realities of living with a more liquid, higher-output stoma afterwards.
Recovery isn’t just about the wound healing well. It’s also about how manageable the stoma feels when you’re tired, sore, and trying to get back to ordinary life.
Sleep is often one of the first things to suffer, especially when you’re learning a new routine and waking to check your pouch. Gentle planning around sleep and rest after cancer surgery can help the body recover and make daytime stoma care feel less overwhelming.
Patients usually focus on pain, movement, and the stoma itself. Relatives often notice something else first: the learning curve. There are new supplies, a new bathroom routine, and a lot of trial and adjustment.
That early phase is rarely neat. Pouches may need changing at awkward times. Clothing may feel strange against the abdomen. Appetite may be patchy. The stoma can also change size in the weeks after surgery as swelling settles, which means your pouch fit may need reviewing.
A calm message I often give patients is this:
At home, this is often the moment the difference between a colostomy and an ileostomy becomes real. You are standing in the bathroom, tired from treatment, looking at the pouch and wondering, “How often will this need attention, and will I ever stop thinking about it?”
For many patients and families, output is the part that shapes the day most clearly.
| Feature | Colostomy | Ileostomy |
|---|---|---|
| Part of bowel used | Colon, or large bowel | Ileum, or small bowel |
| Usual output | Thicker, more formed stool | Looser, more liquid output |
| Typical pattern | Often slower and more formed | Often more frequent and more liquid |
| Early pouch emptying pattern | May be less frequent, depending on routine and pouch type | Often needs more regular emptying, especially early on |
| Main day-to-day concern | Managing thicker stool, wind, and pouch fit | Hydration, skin protection, and higher output |
| Dehydration risk | Usually lower | Higher, especially in the early weeks |
UK stoma service data commonly quoted in patient education highlights the pattern behind this table. Colostomy output is often more solid and lower in volume, while ileostomy output is usually more liquid, emptied more often, and linked with a higher early dehydration risk. One summary of these figures is available in these stoma output statistics.
A colostomy often behaves more like a bowel motion collected in a pouch. That can feel easier to picture. The stool is often thicker, so leaks may be less about speed and more about fit, pancaking, or wind building up in the bag.
An ileostomy is different. The output is usually closer to a thick soup or porridge, and it can keep coming through during the day rather than arriving in one clear “toilet moment”. For a patient recovering from cancer surgery, that can feel tiring at first because the pouch may need emptying more often and the skin around the stoma needs careful protection.
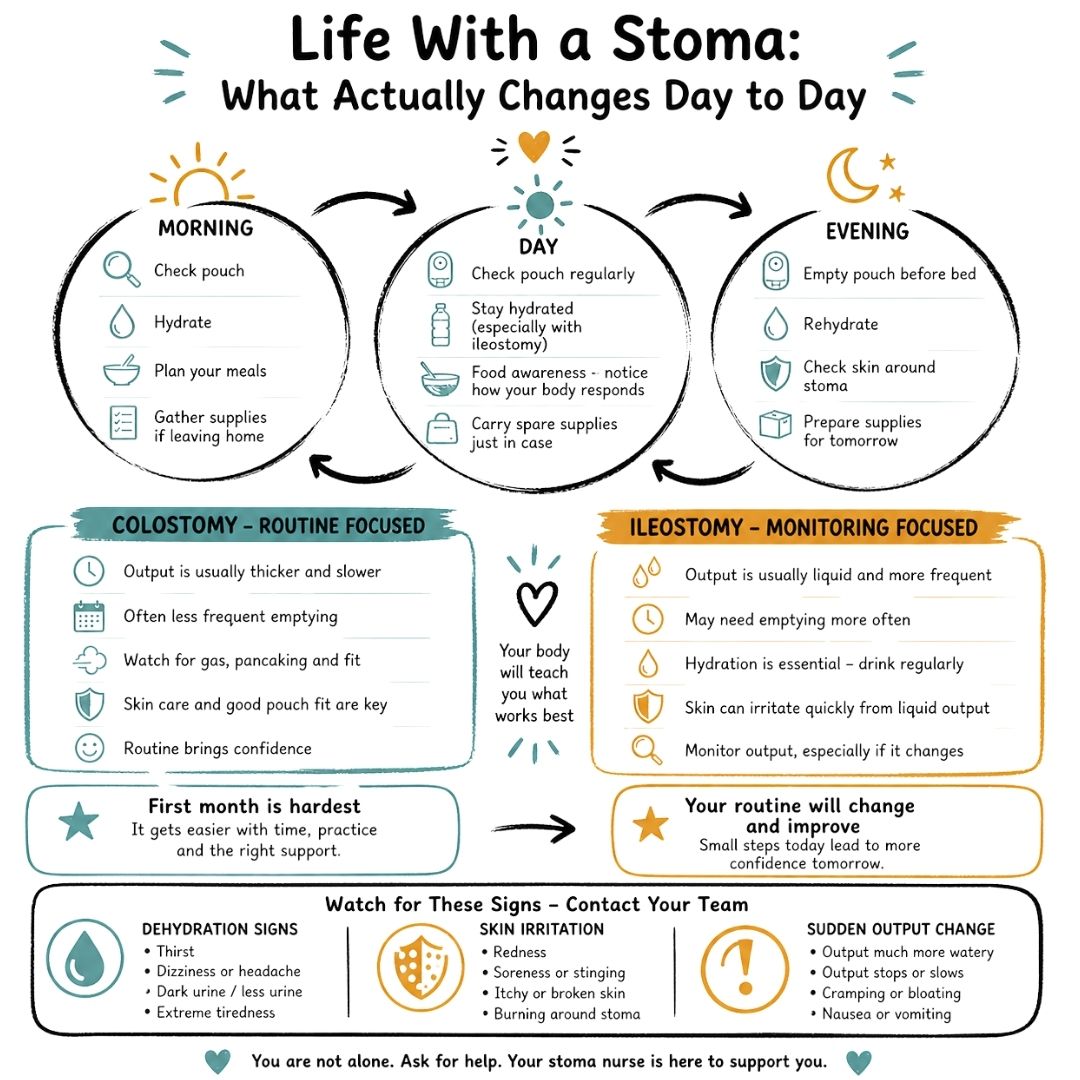
The simplest way to explain it to families is this. A colostomy often asks for routine. An ileostomy often asks for monitoring.
That does not mean life stops. It means the habits are different.
While managing a stoma does not require all-day attention, new checkpoints are built into ordinary life. Before leaving the house. Before a long car journey. Before bed. Sometimes once during the night.
With a colostomy, some people find the day feels more predictable once the bowel settles. With an ileostomy, the pattern may stay more changeable, especially during chemotherapy, after a stomach bug, or when appetite is poor. Caregivers often become part of this routine early on, helping notice when output looks more watery, when the pouch is filling faster than usual, or when the person is too drained to keep up with fluids.
This learning period can affect confidence more than people expect. Patients often worry about leaks in public, smell, intimacy, work meetings, or whether they will feel “normal” in their own clothes again. Those worries are common, and they usually ease as the routine becomes familiar.
Pouch care works best when it becomes boring. That is usually the goal.
Liquid ileostomy output can irritate the skin quickly if there is even a small leak around the stoma. Colostomy output may be gentler on skin, but a poor fit can still cause soreness, itching, and patches of broken skin. If the skin is painful, every pouch change feels harder, and that can knock confidence fast.
Small practical habits help. Emptying before the pouch gets too full. Checking the adhesive after showers. Asking for a stoma nurse review if the stoma changes size or shape. Trying different products if the current system is not giving a good seal. The first setup is rarely the final one.
Many patients notice that output seems tied to what, when, and how they eat. A simple food and output diary can make patterns easier to spot without becoming obsessive. If you are rebuilding confidence with meals, this guide to foods that are easy to digest after surgery can be a helpful starting point, and some patients also like reading broader Gym Snack recommendations for digestive wellness.
For ileostomy patients, fluids deserve close attention. Dehydration can come on faster than many families expect, especially in hot weather, during sickness, or when output suddenly turns very watery. Signs may include thirst, dizziness, headache, dark urine, low urine output, unusual tiredness, or feeling foggy and weak.
If you have an ileostomy and your pouch starts filling far faster than usual, or the output becomes much more watery, contact your clinical team early.
Colostomy patients can still deal with leaks, sore skin, noisy wind, and unpredictable days. Ileostomy patients often have the added burden of watching hydration closely. Neither experience is “easy”, but understanding the pattern helps you plan your days, protect your energy, and get back to family life with more confidence.
Food becomes emotional after bowel surgery. You’re not just eating for pleasure. You’re watching your body for clues. Does that meal cause cramps? Is the pouch filling more quickly? Why did yesterday’s lunch seem fine and today’s didn’t?
That uncertainty is exhausting at first, especially when cancer treatment has already disrupted appetite and energy.
It is often best to think in terms of testing and observing, not rigid perfection. The bowel often needs time to settle, and your personal tolerance matters.
A few principles tend to help:
For broader meal ideas, this guide to a healthy diet for cancer patients can help you build meals around recovery rather than restriction. Some readers also like browsing Gym Snack recommendations for digestive wellness for general gut-friendly food ideas, then adapting them to their own stoma nurse’s advice.
Patients often tell me that the hardest part isn’t the pouch. It’s losing trust in their body.
An ileostomy can add another layer because output may be more active and less predictable. Long-term quality-of-life data reported that ileostomy patients had 22% higher anxiety scores at 12 months post-surgery, often linked to sleep disruption from frequent pouch changes, according to reported long-term quality-of-life findings. The same data noted that family members of ileostomy patients may spend up to 12 more hours per week on support tasks.
Those numbers reflect something families already know. The stoma affects more than the person wearing the pouch. It can alter shopping, cooking, bedtime routines, confidence about leaving home, and who listens out for trouble at night.
Many patients shrink their world after surgery. They eat only a handful of “safe” foods, avoid car journeys, stop social visits, and become hyper-alert to every noise from the pouch.
That stage often eases with experience.
Helpful milestones usually look ordinary:
Later on, practical coaching can be easier to absorb in video form, especially when fatigue makes reading harder:
If food has become a source of fear, ask for specific dietetic or stoma nurse support rather than trying to “work it out” while exhausted.
The aim isn’t to create a perfect bowel routine. It’s to help you feel nourished, safer, and more at home in your body again.
Every stoma type has trade-offs. People often want a simple answer about which one has fewer problems, but real life is more specific than that.
A large analysis found that ileostomy had an advantage in reducing overall enterostomy complications, with an odds ratio of 0.43, according to this multicentre analysis of protective loop stomas. The same analysis reported higher stoma retraction rates in colostomy, 21.6% versus 9.4%, where the stoma pulls back into the abdomen.
That’s useful, but it doesn’t remove the lived burdens that many ileostomy patients face, especially around high output and skin irritation from liquid effluent. Colostomy may have fewer hydration issues day to day, yet some patients struggle more with stoma shape, fit, or retraction.
Some complications are obvious. Others creep in gradually.
Changes that seem small on Monday can become much harder by Friday. Early review usually saves discomfort.
If your stoma was created to protect healing, reversal may be discussed once your team is satisfied that the bowel has recovered and your overall treatment plan allows it. That decision depends on the original surgery, the state of the bowel, any further cancer treatment, and your general fitness.
Reversal is hopeful for many people, but it’s still another operation. It also doesn’t always mean bowel function returns instantly to how it was before. Some patients have temporary urgency, loose stool, or a period of bowel retraining afterwards.
Questions worth asking include:
That kind of clarity helps you prepare for the actual road ahead, not an idealised version of it.
The best choice in colostomy vs ileostomy depends on the job the stoma needs to do.
If the aim is to protect a new bowel join during curative surgery, ileostomy is often considered because it can work well as a diverting stoma and may offer technical surgical advantages in the right setting. If the aim is to relieve symptoms in advanced cancer and keep postoperative burden lower, the balance may shift.
In palliative care for advanced colorectal cancer, one study found lower stoma-related complications with colostomy at 22.4% versus 48.5% for ileostomy, and lower 30-day mortality at 0% versus 9.1%, according to this comparative study of palliative ostomy procedures. In that context, avoiding high-output problems can make a major difference to comfort and day-to-day management.
That’s why the most useful clinic conversation isn’t “Which one is best?” It’s “Which one best fits my situation?”
Bring your priorities into the room. Some patients care most about the chance of reversal. Others care most about simpler day-to-day care, less dehydration risk, or avoiding another emergency admission. Those concerns are clinically relevant, not secondary.
A written list helps, especially when appointments feel rushed. These questions to ask your oncologist can help you frame concerns about goals of treatment, recovery, and what life at home may realistically involve.
Patients often save the most important questions until the very end of an appointment. They’re usually not about surgery technique. They’re about identity, relationships, clothes, movement, and whether life will still feel normal.
It can, but not always in the way people expect.
A 2024 Macmillan Cancer Support study found that 41% of UK ileostomy patients experienced relationship strain linked to fears about liquid output during intimacy, compared with 29% of colostomy patients, according to these reported intimacy findings in ostomy patients. The same source reported higher body image issues in colostomy patients, at 62% versus 48%, linked to larger, more visible stomas.
So the emotional burden can differ. Ileostomy may create more worry about leakage or liquid output. Colostomy may create more concern about appearance under clothes. Neither response is vanity. Both are part of adapting.
Usually, yes. Individuals typically return to walking first, then gradually build up to more activity depending on surgical recovery and medical advice. The pouch should fit securely, and many people find confidence rises once they’ve successfully managed a few ordinary outings.
Start with low-pressure trips. A short walk. A café near home. A visit with someone you trust. Confidence grows from repetition, not from waiting to feel fearless.
Very likely, yes.
Early on, the stoma can feel like the centre of everything. Later, it usually becomes one part of life rather than the whole story. You may still have difficult days. You may still need practical adjustments. But many people reach a point where they plan around the stoma without feeling defined by it.
Ask direct questions. Tell your nurse if you're worried about sex, smell, sleep, body image, or leaving the house. Those are stoma care questions too.
If you need extra support, look for a stoma nurse, your hospital cancer support team, or established bowel cancer and ostomy charities in your area. Talking to someone who understands the lived reality can be as important as any piece of equipment.
We strongly advise you to talk with a health care professional about specific medical conditions and treatments.
The information on our site is meant to be helpful and educational but is not a substitute for medical advice.
What is the colon cancer prognosis? Learn about stages, survival rates, treatment success, and what affects long-term outcomes.
Facing a stage 4 bowel cancer diagnosis? This clear guide explains what it means, how it spreads, treatment options, managing symptoms, and ways to protect your quality of life, empowering you with facts and next steps.
Asking 'what is a colostomy'? This compassionate guide explains the surgery, recovery, stoma care, and how to live fully after a colostomy procedure.