Hearing that you may need lymph node removal can make your stomach drop. Patients often don’t just hear “surgery”. They hear a rush of questions. Has the cancer spread? How much will they remove? Will it hurt? Will my arm or leg swell afterwards? What happens next?
Those questions are normal. They come from the same place as many of the hardest parts of cancer care: uncertainty.
Lymph node removal is one of those procedures that often sounds more alarming than it is, partly because the language around it can feel technical and partly because the reasons for doing it are tied so closely to staging, treatment planning, and fear of spread. When you understand what your team is looking for and how the operation fits into the bigger picture, it usually feels more manageable.
Lymph node removal means a surgeon takes out one or more lymph nodes so they can be examined for cancer cells. Sometimes only a small number are removed. Sometimes a wider group of nodes is taken out. The exact operation depends on the type of cancer, where it started, what scans and biopsies have shown, and what information your team still needs.
For many patients, this happens alongside surgery to remove the main tumour. For others, it’s done to clarify staging, guide radiotherapy or drug treatment, or treat lymph nodes already known to contain cancer.
If you’ve been checking your body constantly and wondering what’s normal, it may help to read about what lymph nodes feel like. That can make clinic conversations less abstract and help you describe symptoms more clearly.
You don’t need to memorise the medical language. You need to understand the purpose of the procedure, what recovery may look like, and which questions matter most for your situation.
The important thing to know at the start is this. Lymph node removal isn’t automatically the same as “the cancer is everywhere”. Very often, it’s a careful way to gather information and tailor treatment while avoiding more surgery than you need.
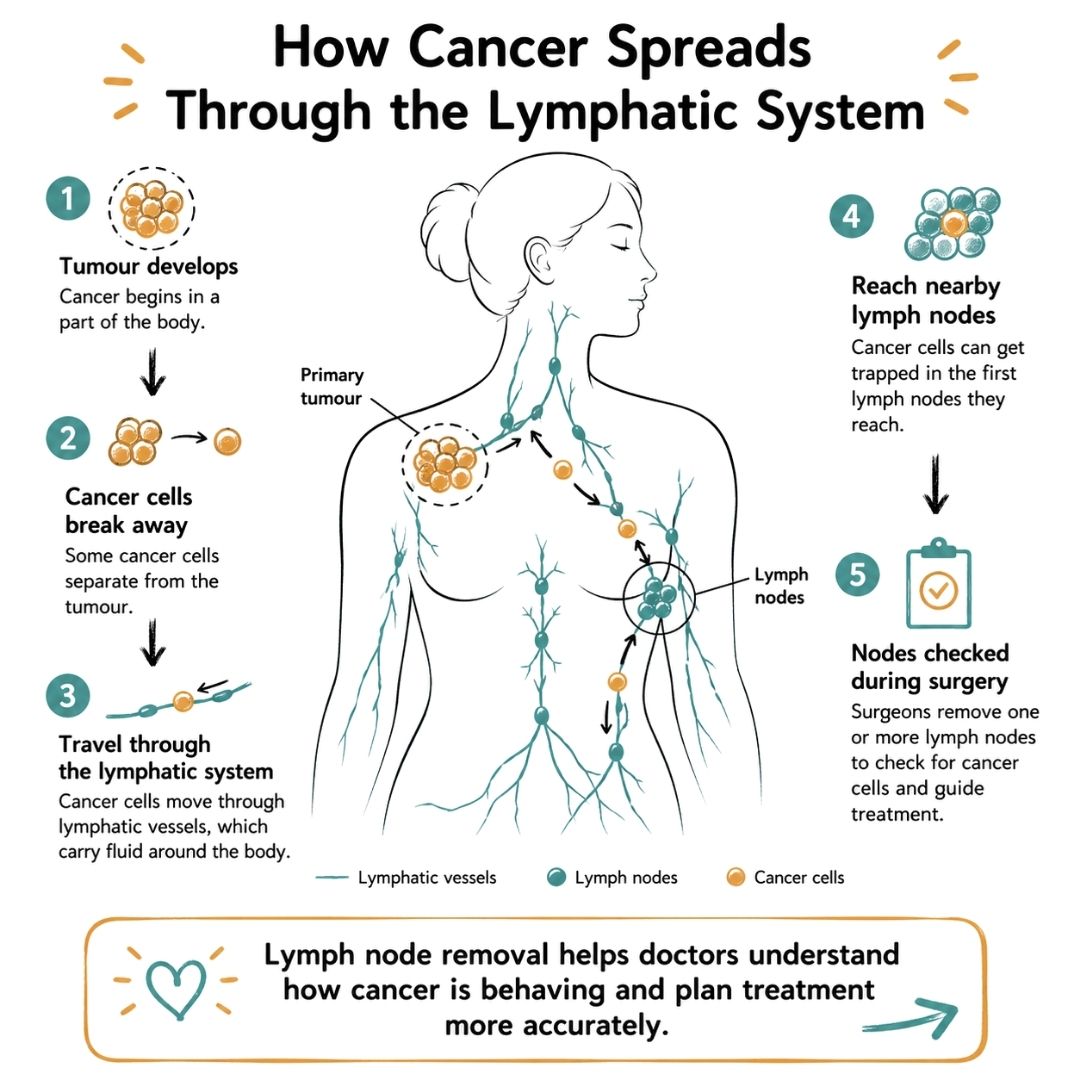
Think of your lymphatic system as a network of tiny roads and checkpoints running through your body. Fluid moves through these channels, and lymph nodes act like filters. They help your immune system notice things that shouldn’t be there, such as infection or abnormal cells.
That’s why doctors pay close attention to them in cancer care. If cancer cells break away from the original tumour, they can sometimes travel through these lymphatic channels and get trapped in nearby nodes.
Lymph nodes are small bean-shaped structures found in groups, including in the neck, armpits, chest, tummy, and groin. Under ordinary circumstances, they help clear waste, germs, and damaged cells from lymph fluid. You can think of them as part of the body’s clean-up and surveillance system.
In cancer, that same filtering job is exactly what makes them important. A nearby node may be the first place where stray cancer cells are detected. That doesn’t tell the whole story by itself, but it gives your team valuable clues.
For some blood cancers and related conditions, testing isn’t about removing a specific node first. Blood work and specialised lab analysis can also help define what’s going on. If your team is investigating lymphoma or leukaemia, a test overview like the DoctorDoc leukemia lymphoma panel can help you understand the sort of laboratory information haematology teams may use alongside scans, biopsies, and clinical assessment.
Your clinicians aren’t interested in lymph nodes out of curiosity. They want to answer practical questions that affect treatment decisions.
A common point of confusion is this. Checking lymph nodes doesn’t always mean removing lots of them. In many cancers, surgeons try to get the information they need with the smallest effective procedure.
Practical rule: The purpose of lymph node removal is usually to guide treatment as accurately as possible while limiting unnecessary harm.
People often worry that removing lymph nodes means the immune system will stop working properly. In most cases, the body still has many other lymph nodes and pathways. The bigger concern after surgery is usually not “losing immunity” in a general sense. It’s the local effect on drainage in the area where nodes were removed, which is why swelling can develop later.
That’s also why supporting your body during treatment matters in a broad sense, including sleep, movement, nutrition, and infection prevention. If you want a patient-friendly overview, this guide on immune system support during cancer treatment is a useful companion.
Not all lymph node removal is the same. Two patients can both be told they’re having “node surgery” and mean very different things.
The simplest way to understand it is this. Sometimes the surgeon checks the first checkpoint. Sometimes they clear a larger section of the route.
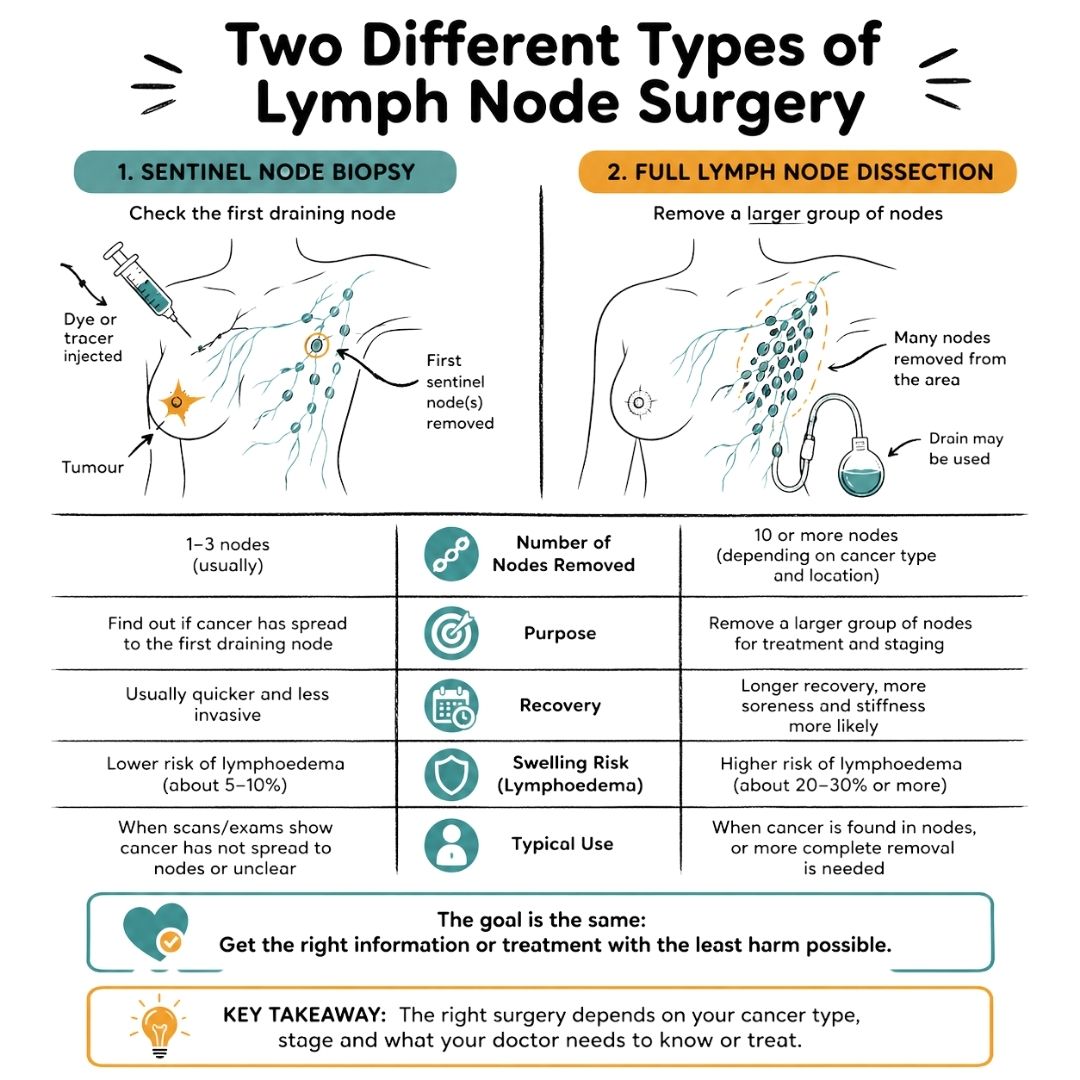
A sentinel lymph node biopsy, often shortened to SLNB, targets the first lymph node or first few lymph nodes most likely to drain fluid from the tumour area. If you imagine a queue, this is like checking the first person or first few people rather than searching everyone in the building.
To identify these nodes, the surgeon uses a tracer such as blue dye, a radioactive tracer, or both. The tracer travels to the first draining node. That helps the surgeon remove the node most likely to show whether cancer has started to travel through the lymphatic system.
This approach is often preferred when it’s suitable because it gathers staging information with less disruption to nearby lymphatic drainage than a larger operation.
A full lymph node dissection removes a larger group of nodes in a defined area. In breast cancer surgery, this may be an axillary lymph node dissection, which involves removing nodes from the armpit region. In UK practice, axillary lymph node dissection involves removing 10 or more lymph nodes from levels I and II in relevant cases, according to the verified data provided.
This is usually considered when cancer is already known to be in the nodes, when there’s a need for more complete clearance, or when the treatment plan calls for wider node removal based on the cancer type and extent.
Because more tissue is removed, the risk of side effects such as stiffness, numbness, and lymphoedema is generally higher than with a sentinel procedure.
| Feature | Sentinel Lymph Node Biopsy (SLNB) | Full Lymph Node Dissection (e.g., ALND) |
|---|---|---|
| Main purpose | Checks the first draining node or nodes for staging | Removes a larger group of nodes for staging and treatment |
| Amount of surgery | Smaller, more targeted | More extensive |
| Typical use | When the team wants key staging information with less surgery | When node involvement is known or broader clearance is needed |
| How nodes are found | Usually with dye, radioactive tracer, or both | Based on known anatomical node groups |
| Effect on drainage | Usually less disruption | Greater disruption, so swelling risk is higher |
| Recovery | Often quicker and simpler | Usually more involved, especially if a drain is used |
The location of lymph node removal depends on where the cancer began.
For example, in penile cancer, inguinal lymph node dissection is a standard operation in the UK for certain stages and targets 8 to 15 nodes per side according to the verified evidence from this PMC review. The same evidence notes that using specific post-operative drains in British audits reduced wound infection from 28% to 9%. That’s a good reminder that the surgery, and the aftercare, are specific to the cancer type.
People often compare notes in waiting rooms or online groups and then feel confused. One person had two nodes removed. Another had many more. That difference doesn’t automatically mean one cancer is worse. It may reflect a different cancer type, location, previous treatment, scan findings, or surgical goal.
If you’re preparing for breast surgery, practical items can make the early recovery period easier, especially if arm movement feels awkward for a few days. This guide to a post-surgical bra after breast surgery can help you think ahead.
A smaller operation isn’t “better” in every situation. The right operation is the one that gives your team the information or treatment effect you need, with the least unnecessary impact on your body.
Most patients cope better when they know the sequence of events. The experience usually feels less frightening when it’s broken down into ordinary steps.
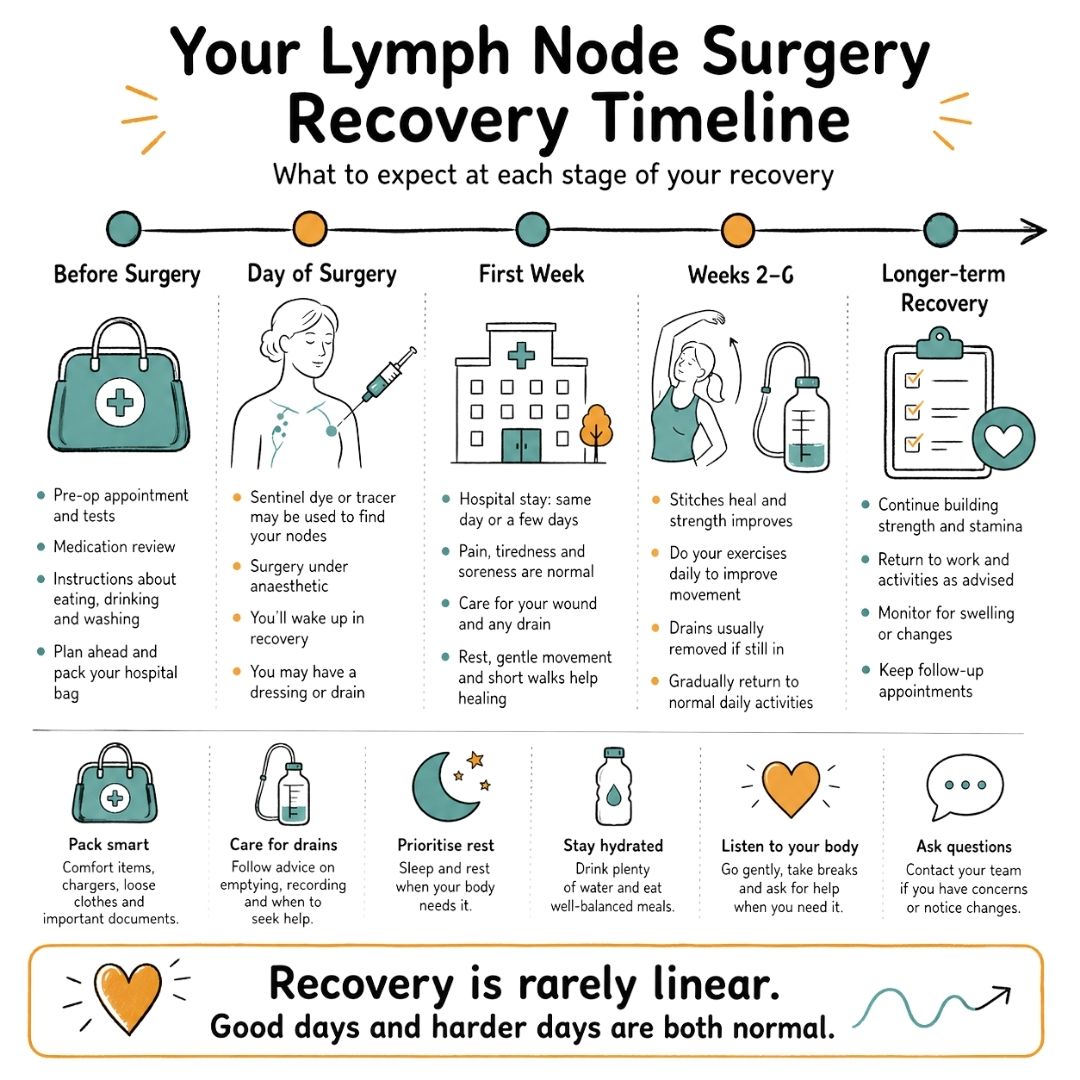
In the days before surgery, your team will give you instructions about eating, drinking, medicines, washing before the procedure, and when to arrive. If your operation includes sentinel node mapping, you may also be told about dye or tracer injections used to identify the correct nodes.
You’ll usually have a pre-assessment appointment. That may include blood tests, a medication review, and time to discuss allergies, previous anaesthetic problems, or health conditions such as diabetes, asthma, or heart disease.
A practical bag packed in advance saves a lot of last-minute stress. Many patients find it helpful to use a hospital bag checklist for cancer treatment so they remember chargers, lip balm, loose clothing, important documents, and anything they’ll want when they’re tired afterwards.
You’ll change into a hospital gown, meet members of the theatre team, and confirm what operation is planned. The surgeon may mark the surgical site. The anaesthetist will talk you through the anaesthetic and pain relief plan.
Then there’s a lot of waiting mixed with very short bursts of action. You’re taken to theatre, given the anaesthetic, and the next thing many people remember is waking in recovery.
If your procedure is a sentinel biopsy, the number of nodes removed can vary. In a UK study from Edinburgh, surgeons removed an average of 2.2 sentinel nodes, rising to 3.5 nodes in patients who had chemotherapy before surgery, according to the published analysis. That’s one reason your operation may not look exactly like someone else’s on paper.
When you wake, you may notice a dressing, some tightness, and perhaps a small drain depending on the operation. Drains are soft tubes that remove fluid from the surgical area into a collection bottle. Not everyone needs one, but if you do, the nursing team will show you how it works and what to watch for.
Common early experiences include:
Some people go home the same day. Others stay longer, especially if the surgery was more extensive, a drain is in place, or the main cancer operation was done at the same time.
If you wake up feeling emotional, shaky, or tearful, that’s not unusual. Anaesthetic, relief, fear, pain medicine, and pure exhaustion can all hit at once.
The operation itself is only part of the story. After surgery, the removed lymph nodes go to pathology. Specialists examine them under a microscope to see whether cancer cells are present.
Those results help your team decide whether you need no further node treatment, more surgery, radiotherapy, systemic treatment, or follow-up. Waiting for those results is often one of the hardest parts, because physically you’re recovering while mentally you’re still waiting for the next answer.
The first side effects after lymph node removal are usually local and manageable. Pain, bruising, stiffness, pulling, altered sensation, and tiredness are common. They don’t mean anything has gone wrong on their own. They usually reflect healing.
The side effect patients worry about most, and rightly ask about, is lymphoedema. That’s swelling caused by a build-up of lymph fluid when the drainage system has been disrupted.
When lymph nodes are removed, or treated with surgery and radiotherapy, the body sometimes struggles to move fluid through that area as efficiently as before. The result can be swelling in an arm, breast, chest wall, leg, groin, or nearby tissue, depending on where treatment happened.
Communication about this risk is often patchy, even though it’s a major patient concern. Verified evidence also shows that less invasive surgery can make a real difference. Moving from full dissection to sentinel-node-only approaches has been associated with a drop in lymphoedema incidence from around 25% to 7% in the evidence summarised by Breastcancer.org.
That doesn’t mean sentinel surgery carries no risk. It means the extent of surgery matters, and asking whether a less invasive option is appropriate is a sensible, practical question.
Lymphoedema doesn’t always announce itself dramatically. Early changes can be subtle.
If you notice any of those, tell your cancer team or GP promptly. Early assessment matters.
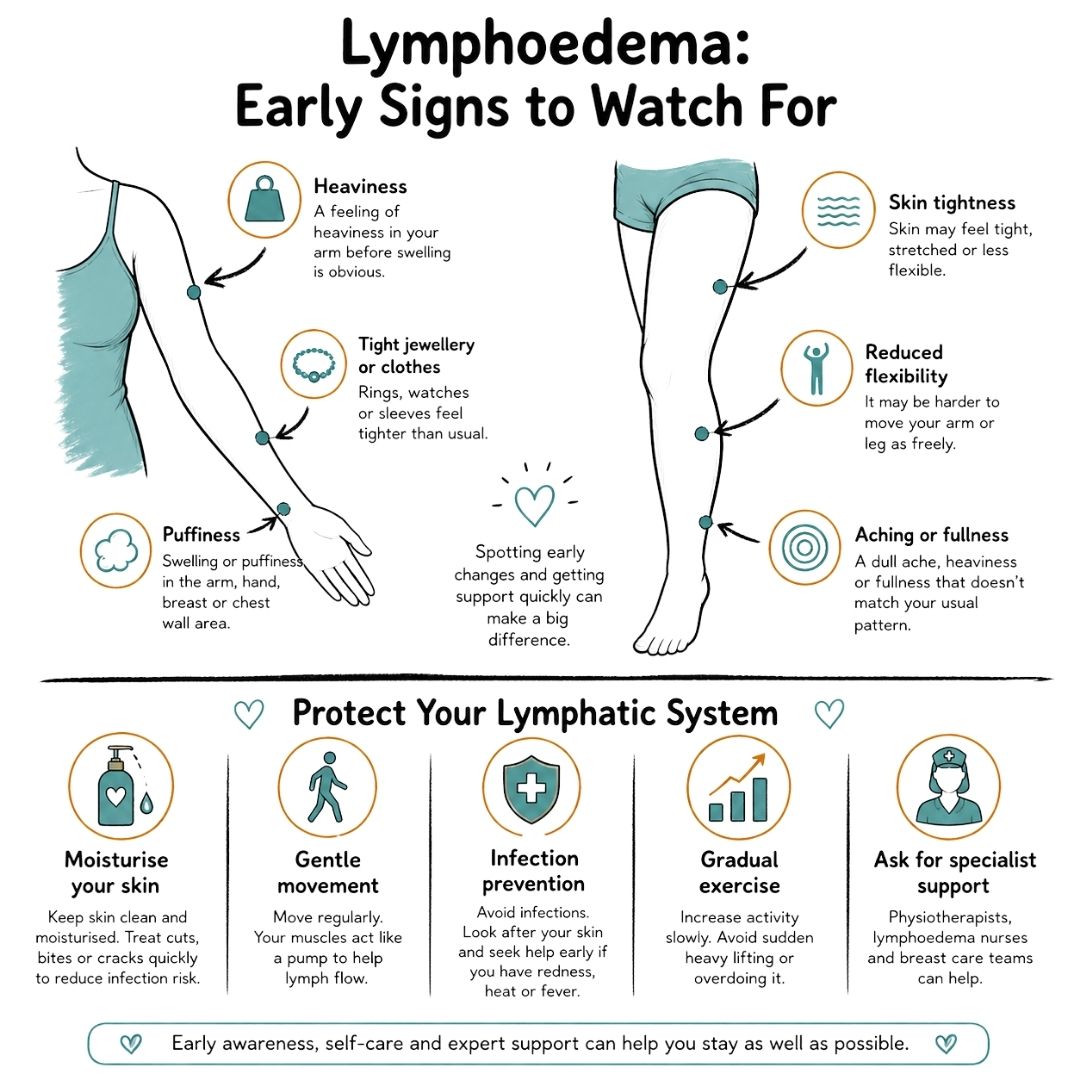
You can’t control every risk factor, but you can reduce strain on the affected area and spot problems sooner.
If you’d like a practical overview of how rehabilitation fits in, this article on lymphedema treatment through PT explains the role of physical therapy in plain language.
For a broader patient guide focused on oncology care, understanding and managing lymphoedema in oncology patients is another useful reference.
A short explainer can also make the topic easier to visualise:
Some centres also discuss newer preventive techniques, including procedures designed to support lymphatic drainage at the time of surgery. These approaches may not be available everywhere, and patient awareness is still limited, but it’s reasonable to ask whether your surgical team offers any preventive strategy or referral pathway for higher-risk patients.
The best time to ask about lymphoedema is before surgery, not only after swelling starts.
Contact your team quickly if you develop sudden swelling, redness, increasing warmth, fever, wound leakage, or pain that is rapidly worsening. Those symptoms can signal infection or another post-operative problem that needs prompt treatment.
Recovery after lymph node removal is rarely a straight line. One day you’ll feel fairly capable. The next you may feel sore, tired, or emotional again. That’s frustrating, but it’s common.
In the first few days, the priorities are pain control, wound care, gentle movement, hydration, and rest. You may need help with washing, dressing, meal preparation, or lifting things, especially if surgery involved the armpit or groin.
Driving, housework, and carrying shopping often need to wait until you can move comfortably, react safely, and follow your surgeon’s advice. If a drain is in place, that can affect what feels manageable too.
This is usually the phase where stiffness becomes more noticeable. Many patients feel better generally but realise their shoulder, arm, leg, or neck doesn’t move quite normally. That’s where prescribed exercises matter. They help restore range of motion and reduce the “protective hunch” people often adopt after surgery.
A few practical anchors help during this stage:
“Back to normal” means different things for different people. Someone with a desk job, straightforward healing, and a small node procedure may return sooner than someone recovering from broader surgery plus chemotherapy or radiotherapy.
If you or your family need more hands-on support during recovery, especially when fatigue or limited mobility makes day-to-day tasks hard, services such as Caremark Bromley live-in care show the kind of practical home support some patients explore after hospital discharge.
Healing is measured less by a calendar date and more by what your body can do safely, comfortably, and consistently.
It also helps to accept that emotional recovery often lags behind physical healing. Many people cope well during the rush of appointments, then feel more vulnerable once they’re home and expected to “get on with it”. That doesn’t mean you’re not recovering. It means you’re human.
Appointments move quickly. It helps to bring a written list, take notes, and ask someone to come with you if possible. Good questions don’t annoy your team. They help your team tailor care and help you make informed decisions.
One reason this matters is that medical guidance changes. Verified evidence shows that for some women over 70 with early-stage, hormone-positive breast cancer, lymph node surgery may be safely omitted, yet many eligible patients still still undergo it, as discussed in this PubMed record. So it’s worth asking whether the planned approach still matches the latest evidence for your situation.
Useful questions include:
Bring the list out in the appointment. Patients often apologise for doing that. There’s no need.
Lymph node removal sits at the crossroads of diagnosis, treatment planning, and recovery. It can sound frightening at first, but the procedure usually makes more sense once you understand its job. Your team is trying to learn how cancer is behaving, treat what needs treating, and avoid unnecessary surgery when possible.
Knowledge helps, but support matters just as much.
If you need practical and emotional help, you can explore the patient resources, workshops, and guidance available through Cancer Care Parcel. When available, the organisation also offers practical post-treatment support items, including a Cancer Care Parcel designed for people going through recovery.
You may also want to keep trusted organisations close by for ongoing information and support, including Macmillan Cancer Support and Cancer Research UK.
If you’re facing lymph node removal soon, write down your questions today, bring them to your next appointment, and ask for clear answers in plain language. You deserve to understand what’s happening to your body and how to protect yourself during recovery.
We strongly advise you to talk with a health care professional about specific medical conditions and treatments.
The information on our site is meant to be helpful and educational but is not a substitute for medical advice.
Understand metastasis and breast cancer with our clear guide. Learn about common symptoms, modern treatments, and how to navigate life after a diagnosis.
My appearance has definitely changed over the past twelve months that’s for sure but I’m getting to like the new me especially when I’m pain free.
A practical, evidence-based guide to Breast Cancer Awareness Month covering symptoms, screening, early detection, supportive communication, inclusive awareness, and meaningful ways to help people affected by breast cancer.
