Consider two people diagnosed with the same cancer at the same stage.
One lives in a city, has stable financial resources, easy access to specialist centres, and strong social support. Their diagnosis is followed quickly by referral, staging, and coordinated treatment.
The other lives in a rural area, is under financial pressure, belongs to an ethnic minority group, and must travel long distances for every appointment. Each step in their care requires more time, more cost, and more effort.
The cancer may be biologically similar. The lived experience of care is not.
These differences are not exceptions. They reflect how healthcare systems are structured.
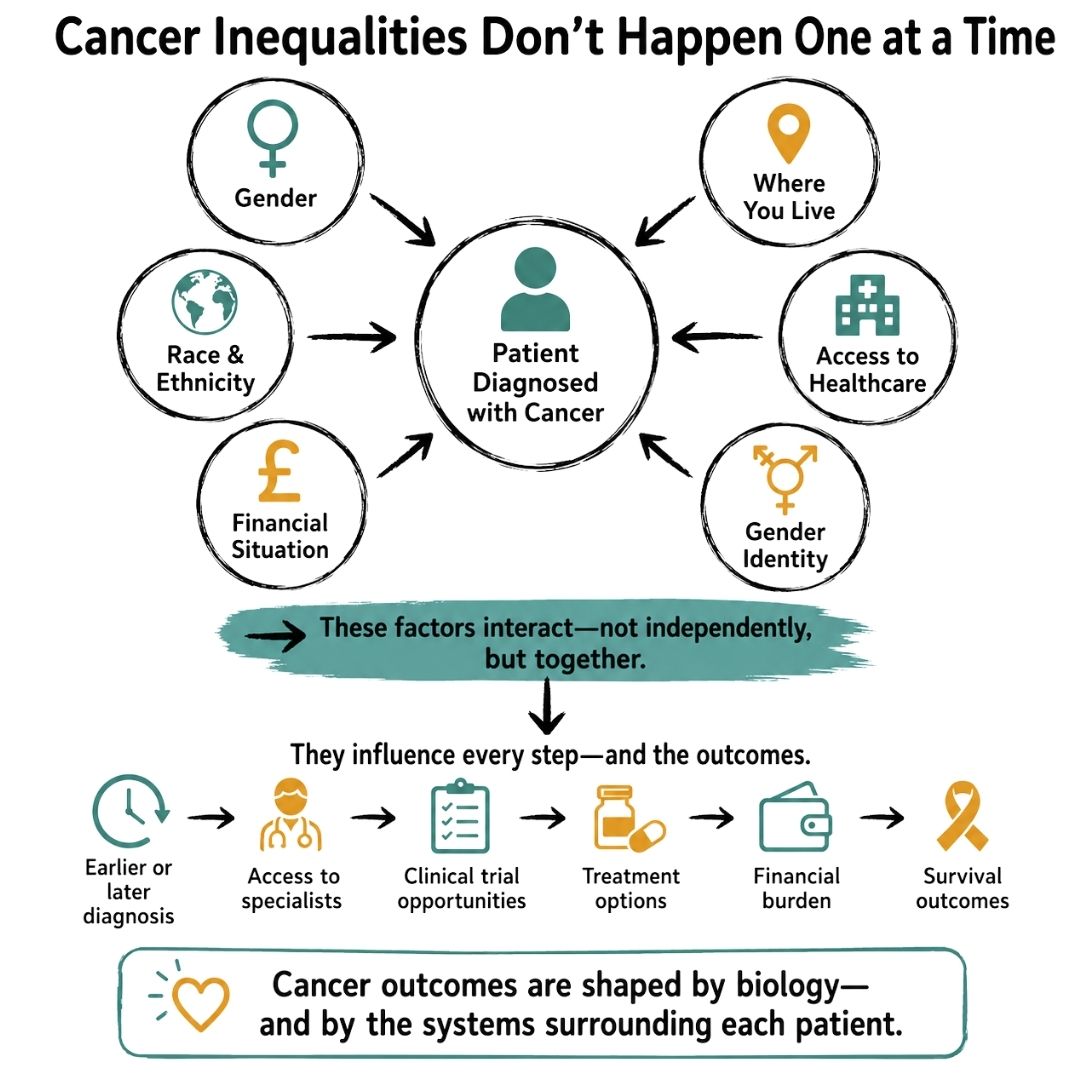
Cancer inequalities are often studied one dimension at a time—race, gender, age, income, or geography.
But real patients do not experience life in separate categories.
Multiple disadvantages often coexist and interact. A person may face financial strain, live far from specialist services, and belong to a marginalised community. These factors do not act independently—they reinforce each other across the cancer journey.
This compounding effect is central to understanding modern cancer inequities.
Women have historically been underrepresented in clinical research, leading to persistent gaps in evidence regarding sex-specific differences in disease biology, treatment response, and toxicity profiles.
As a result, even before considering other social or structural factors, the evidence base itself is not fully balanced.
When additional structural disadvantages are present—such as socioeconomic hardship, racial or ethnic inequity, geographic isolation, or gender identity–related barriers—they do not exist in isolation. Instead, they tend to interact and deepen existing gaps in access and outcomes.
Intersectionality describes how different aspects of a person’s life and identity interact to shape their experience of health and healthcare.
In oncology, this means that inequities are not produced by a single factor. They emerge from overlapping systems—social, economic, and healthcare-related.
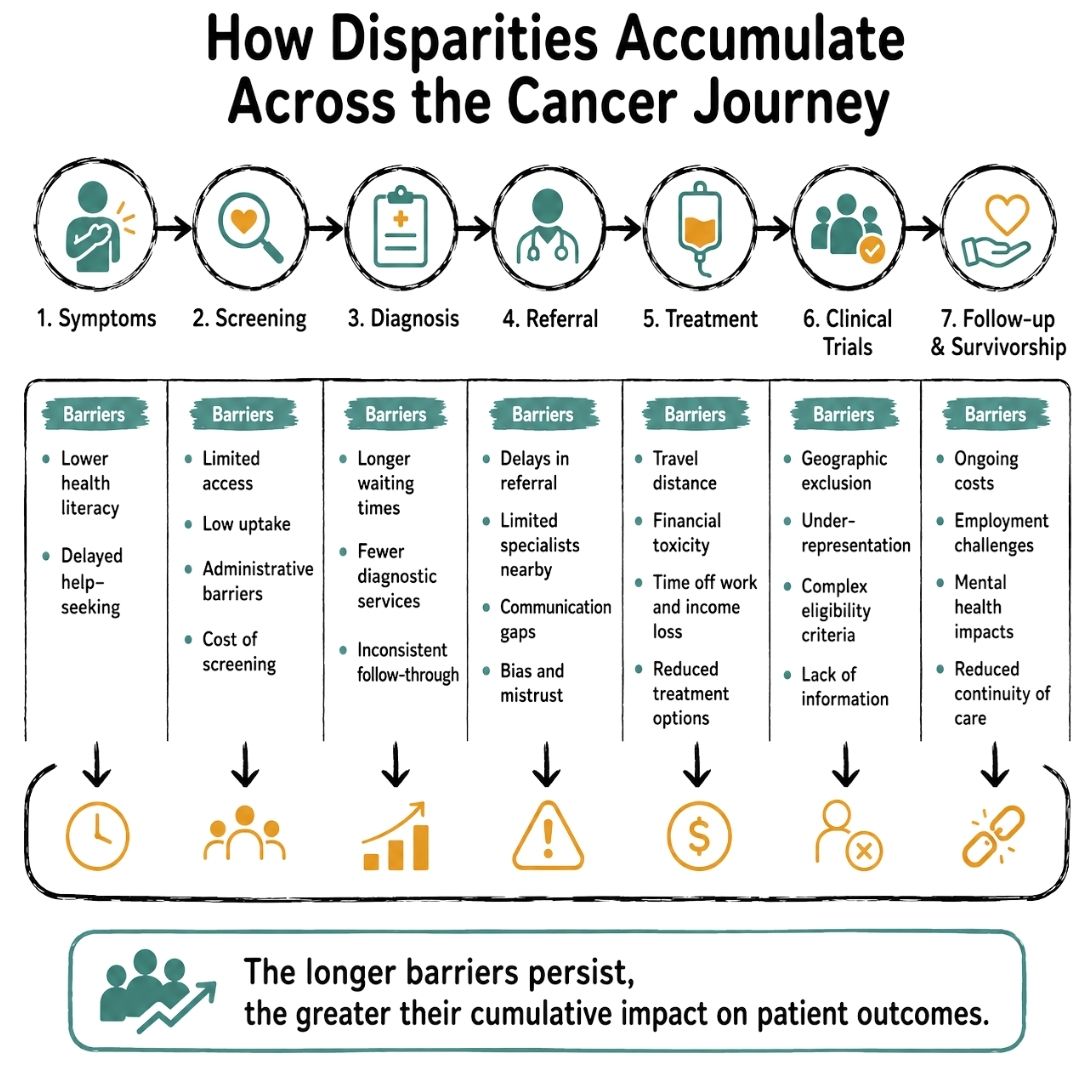
These barriers can influence every stage of care:
Importantly, these effects are not simply additive. They interact and compound over time.
Racial and ethnic disparities in cancer outcomes remain well documented.
Black patients continue to experience higher mortality in several common cancers, including breast, colorectal, prostate, and lung cancer.
These differences are not explained by tumour biology alone.
Delayed diagnosis, unequal access to screening, differences in treatment pathways, underrepresentation in clinical trials, and broader systemic barriers all contribute.
Women have historically been underrepresented in clinical research, limiting the strength of evidence available to guide sex-specific clinical decisions.
Differences in symptom recognition, diagnostic delay, and healthcare engagement can also contribute to variation in outcomes across tumour types.
Socioeconomic status remains one of the strongest predictors of cancer outcomes.
A key mechanism linking socioeconomic disadvantage to worse outcomes is financial toxicity.
Financial toxicity refers to the financial burden and distress experienced by patients as a result of cancer diagnosis and treatment (10). This includes:
Cancer treatment often disrupts employment. Some patients are unable to return to previous work levels, while others experience long-term reductions in earning capacity.
These effects are particularly important in already marginalised populations.
Transgender and gender-diverse people experience higher rates of employment discrimination and income instability compared with the general population. After a cancer diagnosis and treatment, these existing structural vulnerabilities may reduce the likelihood of sustained employment or financial recovery, increasing susceptibility to financial toxicity (11,12).
Financial toxicity therefore reflects not only the cost of care, but also how illness interacts with broader social and economic structures.
Where a person lives continues to strongly influence their cancer journey.
Patients in rural or remote areas often face:
These barriers frequently overlap with socioeconomic disadvantage, further compounding inequities.
Transgender and gender-diverse people may experience healthcare systems that are not fully aligned with their needs. This can include stigma, discrimination, administrative barriers, and gaps in provider training or system design.
These factors may influence:
Cancer screening guidance increasingly recommends organ- and anatomy-based approaches, ensuring that preventive care is aligned with individual clinical needs rather than assumptions based on gender markers (13).
However, limitations in electronic health records and inconsistent documentation of relevant anatomy can still result in gaps in preventive care and follow-up (12).
The central issue is not identity, but whether systems are structured to reliably deliver appropriate care to all patients.
Recognising disparities is only the first step. The challenge lies in changing how care is delivered.
Patient navigation programmes have been shown to improve screening uptake, reduce delays, and support treatment initiation, particularly in underserved populations (14,15).
Clinician education on implicit bias may improve communication, trust, and engagement in care.
Together, these interventions shift responsibility away from patients navigating complex systems alone and toward healthcare systems actively supporting equitable access.
Cancer care is advancing rapidly, with major improvements in diagnosis, treatment, and survival.
But progress is not experienced equally.
Disparities related to gender, race, socioeconomic status, geography, and gender diversity rarely occur in isolation. They overlap, interact, and accumulate across the cancer journey.
Without intentional system-level change, there is a real risk that advances in oncology will continue to benefit those already best positioned to access them.
The central question is therefore not only how far oncology has progressed—but who is still being left behind.
We strongly advise you to talk with a health care professional about specific medical conditions and treatments.
The information on our site is meant to be helpful and educational but is not a substitute for medical advice.
Find cancer support for family with emotional, practical, and financial resources to navigate this journey together.
Cancer Dehydration Is A Risk For People Undergoing Cancer Treatments, This Can Be Life-Threatening If Left Untreated. Find Out More From Cancer Care Parcel.
Learn Key Strategies For Thriving After Cancer. Explore Holistic Approaches To Improve Well-Being During And After Treatment.
