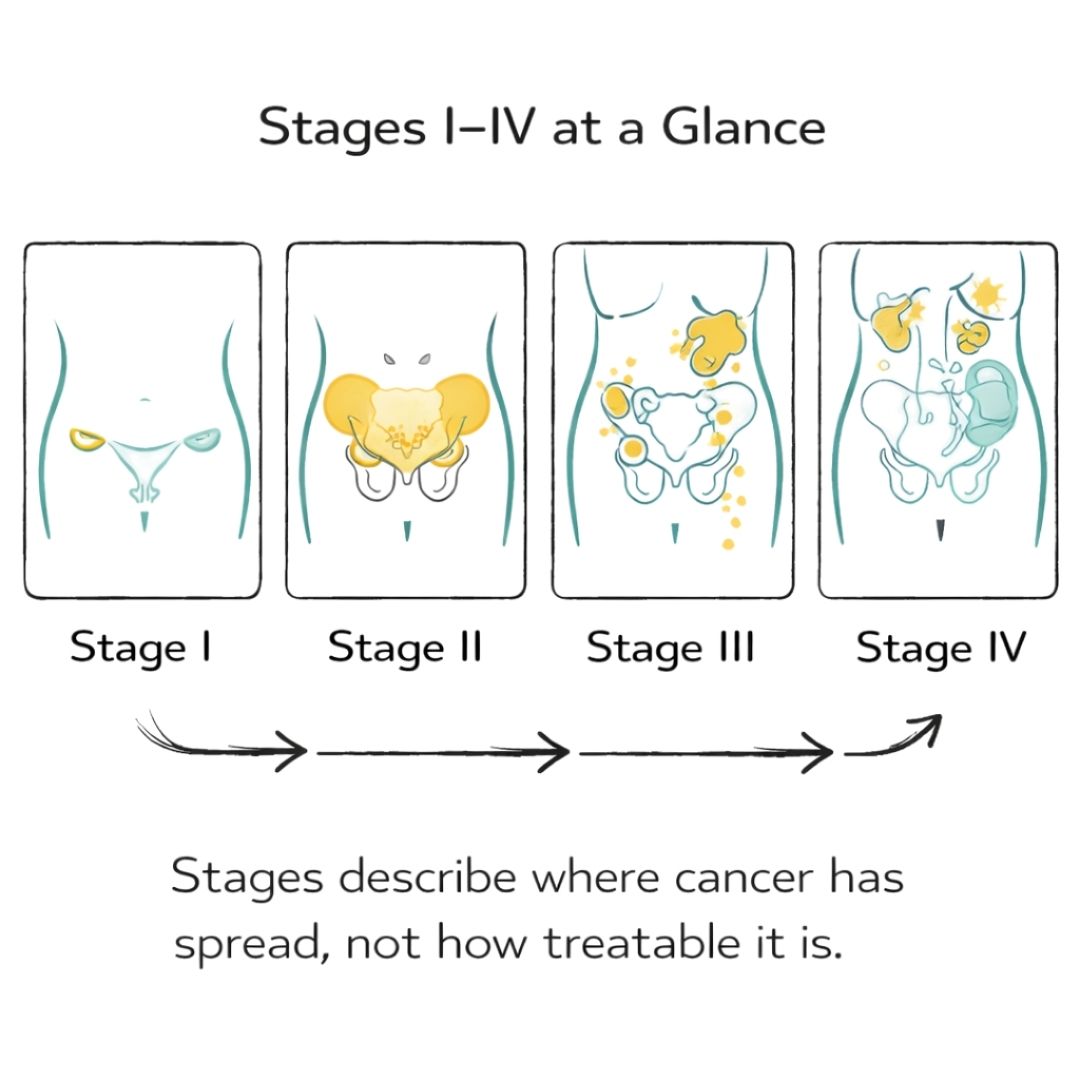
When you first hear the words "ovarian cancer," it can feel like your world has been turned upside down. Suddenly, you're faced with a barrage of medical terms like 'staging' and 'prognosis' that can add to the confusion and anxiety. The stages of ovarian cancer, which run from Stage I to Stage IV, are simply the system doctors use to describe where the cancer is and how far it has spread. Getting your head around your specific stage is a crucial first step in understanding what comes next and building your treatment plan.
It’s completely normal to have a million questions racing through your mind after a diagnosis. The information your care team gives you initially is all about creating a clear picture of your unique situation, and staging is right at the heart of that conversation.
Think of cancer staging as a detailed map that helps navigate the road ahead. It shows your medical team the exact starting point of the cancer, its size, and whether it has travelled to other areas of your body. This insight is absolutely essential for plotting the most effective route forward.
Staging isn't just a clinical label; it serves several really important roles in your cancer care. It provides a common language for doctors everywhere, making sure a Stage II diagnosis in London means the same as one in Los Angeles. This global consistency is vital for research and improving treatments for everyone.
For you, personally, staging is most important because it helps to:
Staging is the bedrock of your treatment strategy. It takes a complex and frightening diagnosis and turns it into a clear, actionable plan, giving you and your team a sense of direction during a very challenging time.
Learning about the different stages really drives home just how critical it is to recognise symptoms early on. Ovarian cancer has a reputation for being a "silent" disease, which is why it's often diagnosed at a later, more advanced stage. This can have a major impact on the prognosis.
The number of women diagnosed with ovarian cancer varies globally, but the challenge of late diagnosis is widespread. This stark reality is a powerful reminder of why we need to be aware of persistent symptoms like bloating, pelvic pain, or feeling full quickly. Catching these signs early can make all the difference. For a more detailed look at what to watch out for, you can read our guide on the symptoms of ovarian cancer.
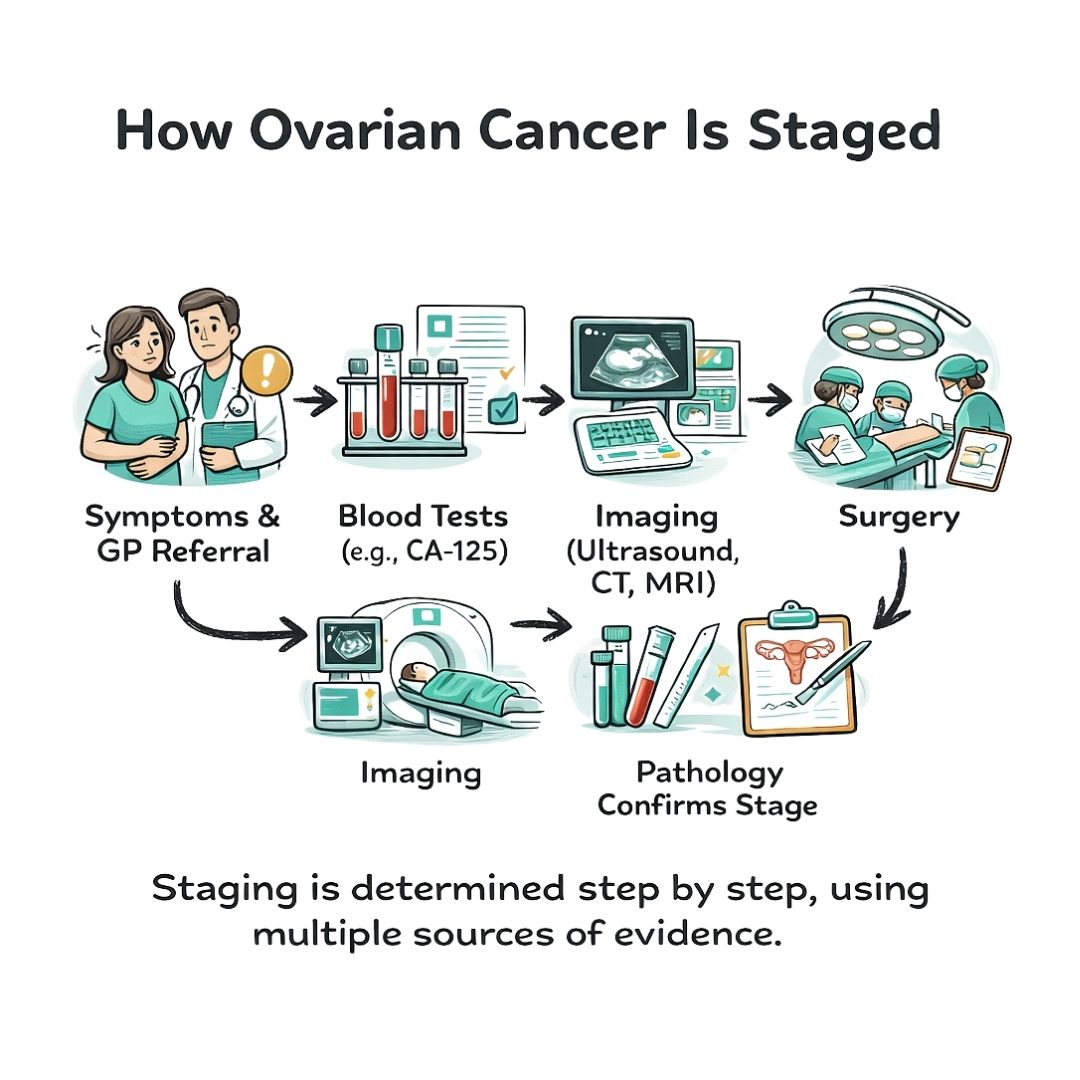
Figuring out the precise stage of ovarian cancer is a bit like a detective piecing together clues. Your medical team will use a combination of different tests and procedures to build a complete picture of the cancer—where it is and how far it might have spread. This methodical process is absolutely essential for creating a treatment plan that’s right for you.
The diagnostic journey usually starts with a physical examination, including a pelvic exam, to feel for any lumps or other abnormalities. From there, your doctor will likely recommend more specific tests to get a clearer view.
Before any surgery is considered, doctors use non-invasive methods to get their first look inside your body. These initial steps are crucial, as they guide the entire next phase of diagnosis and treatment planning.
Blood tests are often one of the first ports of call. You may have heard of the CA-125 test, which measures a specific protein in the blood. Levels of this protein can be higher in women with ovarian cancer, but it’s not a standalone diagnostic tool—other, non-cancerous conditions can also cause it to rise. Still, it provides a very valuable piece of the puzzle.
Alongside blood work, imaging scans are fundamental. These technologies create detailed pictures of your internal organs, letting doctors see the size and location of any tumours. The most common scans include:
These initial tests give your doctors a provisional or "clinical" stage, but the final, definitive stage is almost always confirmed through surgery.
Surgery isn't just a treatment; it's the gold standard for accurately staging ovarian cancer. During the operation, a specialist surgeon, known as a gynaecologic oncologist, can directly see exactly how far the cancer has spread within the pelvis and abdomen.
The surgeon will take small tissue samples, or biopsies, from the ovaries, lymph nodes, and any other areas that look suspicious. These samples are then sent straight to a pathologist, a doctor who specialises in diagnosing diseases by examining tissue under a microscope. Their report provides the final, crucial details about the cancer.
A pathologist's analysis confirms not just the presence of cancer, but also its specific type and grade. This microscopic examination is what turns suspicion into a concrete diagnosis and provides the definitive information needed for accurate staging.
Once all the information from exams, scans, surgery, and pathology reports is in, your doctors use a formal staging system to classify the cancer. Two main systems work together to provide a standardised, universally understood description.
The FIGO System: Developed by the International Federation of Gynaecology and Obstetrics, this is the primary system used for gynaecological cancers. It uses Roman numerals (I, II, III, IV) to describe the extent of the cancer's spread.
The TNM System: This system adds another layer of detail and corresponds directly to the FIGO stages.
Together, FIGO and TNM create a comprehensive diagnosis that guides your care team in selecting the most effective treatments. This thorough, step-by-step process ensures your treatment plan is based on the most accurate and detailed information possible.
Here is the rewritten section, designed to sound like it was written by an experienced human expert.
Receiving a Stage I ovarian cancer diagnosis means the cancer has been caught at its earliest, most treatable point. This is the best-case scenario for a diagnosis, and it comes with an excellent prognosis.
Put simply, Stage I means the cancer is confined to one or both ovaries. It hasn't spread anywhere else. Because the disease is localised, treatment can be incredibly effective. In fact, the five-year survival rate for Stage I ovarian cancer is over 90%, a statistic that offers real hope and underscores just how crucial early detection is.
To get an even clearer picture and fine-tune treatment plans, doctors classify Stage I into three distinct substages: IA, IB, and IC. Think of these as more detailed descriptions of exactly what’s happening inside.
That last point, Stage IC, is an important distinction. If cancer cells have spilled into the abdomen, even on a microscopic level, there’s a slightly higher chance the cancer could return. This detail helps your oncology team make critical decisions about what should happen after surgery.
Surgery is the cornerstone of treatment for Stage I. The operation has two main objectives: first, to officially confirm the stage by taking samples from nearby tissues, and second, to remove all visible cancer. This typically involves removing the affected ovary (or both), the fallopian tubes, and the uterus.
Whether you need more treatment after surgery depends entirely on the substage and the tumour’s grade (a measure of how aggressive the cells appear under a microscope). For someone with a low-grade Stage IA or IB tumour, surgery alone may be all that’s required.
For anyone diagnosed with Stage IC or a high-grade Stage I cancer, chemotherapy is almost always recommended. This is considered an 'adjuvant' or preventative therapy. Its job is to track down and destroy any stray cancer cells that might be lingering, significantly lowering the odds of a recurrence down the road.
While any cancer diagnosis is unsettling, a Stage I diagnosis represents the most optimistic starting point. It’s a powerful reminder to always listen to your body and speak to a doctor about any symptoms that feel out of the ordinary. Catching ovarian cancer this early gives you the very best chance for a full recovery and a healthy future.
As we move past the earliest stage, we get to Stage II and Stage III ovarian cancer. This is a significant point in the journey because it means the cancer is no longer neatly contained within the ovary or ovaries. It has started to spread into the surrounding areas, which naturally calls for a more involved treatment plan.
To picture this, think back to our garden analogy. If Stage I cancer is like a single plant growing tidily in its pot, then Stages II and III are what happens when its roots start pushing out of the bottom and spreading into the nearby soil. The cancer is no longer an isolated issue; it’s starting to affect the immediate environment.
In Stage II, the cancer has grown outside of the ovary (or ovaries) and into other tissues within the pelvis. It’s moved beyond its "pot," but it's still confined to the immediate "garden bed" of the pelvic region.
This stage is broken down a bit further for more precision:
The crucial takeaway for Stage II is that the cancer is still completely contained within the pelvic cavity. Treatment nearly always involves surgery to remove the cancerous tissue, followed by chemotherapy to track down and eliminate any cells that have moved into these neighbouring areas.
Stage III marks a more advanced point. Here, the cancer has spread beyond the pelvis and into the abdominal cavity or has reached nearby lymph nodes. In our garden analogy, the roots have now travelled into the wider garden and may have even tapped into the watering system (the lymph nodes).
A Stage III diagnosis means the cancer is no longer confined to the pelvis. It has moved into the upper abdomen, potentially affecting the lining of the abdomen (the peritoneum) or spreading to the surface of organs like the liver or spleen.
This stage has several sub-stages (IIIA, IIIB, and IIIC) that describe exactly how far the cancer has travelled. For instance, Stage IIIA might involve microscopic deposits in the abdomen, while Stage IIIC means there are larger tumour deposits (over 2cm) or the cancer has reached regional lymph nodes. The spread of cancer to the peritoneum is a key factor here. You can learn more about this specific aspect in our guide on primary peritoneal cancer.
For both Stage II and especially Stage III, a critical operation called debulking surgery (or cytoreductive surgery) becomes a cornerstone of treatment. The main goal is simple but vital: to remove as much of the visible tumour as physically possible. Surgeons often call this achieving "optimal debulking."
This is a highly specialised and often long procedure performed by a gynaecological oncologist. The surgeon aims to leave no visible tumour behind, or at the very most, only tiny deposits smaller than 1 centimetre.
So, why is this so important? The less cancer that remains after the operation, the better the follow-up chemotherapy can work. It has a much smaller, and often only microscopic, amount of disease to target. Successful debulking is one of the single most important factors influencing the prognosis for women with advanced-stage ovarian cancer. After surgery, a course of chemotherapy is the standard next step to destroy any lingering cancer cells and lower the risk of it coming back.
Stage IV is the most advanced of the stages of ovarian cancer, and it means the cancer has travelled beyond the abdomen to distant parts of the body. This is also called metastatic cancer. Receiving this diagnosis can feel overwhelming, but it's crucial to know that treatment is still absolutely an option.
At this point, the focus of care often shifts. While a cure becomes less likely, the goals pivot towards managing the cancer's growth, easing symptoms, and preserving the best possible quality of life. Many people live for years with advanced cancer, learning to manage it much like a chronic illness.
Even within Stage IV, there are distinctions that help your care team get a more precise picture of the cancer's spread. This detail is vital for tailoring treatments to your unique situation.
Stage IVA: This means cancer cells have been found in the fluid that can build up around the lungs (a malignant pleural effusion). The cancer hasn't yet spread into solid organs far from the pelvis.
Stage IVB: In this case, the cancer has reached the inside of distant organs. This could include the liver or spleen, the lungs themselves (not just the fluid), bones, or lymph nodes outside the abdomen, like those in the neck or groin.
This distinction matters. Where the cancer has spread directly influences the symptoms you might have and helps your doctors decide on the most effective treatment strategies. To understand this in more detail, you can read our guide on what it means to have metastatic cancer.
When ovarian cancer reaches Stage IV, the treatment plan is highly personalised. It becomes less about a single cure and more about a long-term strategy to control the disease and minimise its impact on your day-to-day life.
The main treatments often include:
At Stage IV, the goal is to manage the cancer as a long-term condition. The focus is on balancing the effectiveness of treatments with your personal comfort and well-being, ensuring you can continue to live as fully as possible.
Surgery is used less often as a primary treatment in Stage IV. However, it might still be recommended to relieve a specific symptom, such as removing a tumour that’s causing a blockage. As the cancer journey progresses, understanding all the support available is key. This might include learning about what to expect from hospice care, which provides compassionate, comfort-focused support when curative treatments are no longer the primary goal. Above all, your care team’s priority is to create a plan that honours your wishes and helps you maintain a sense of control and hope.
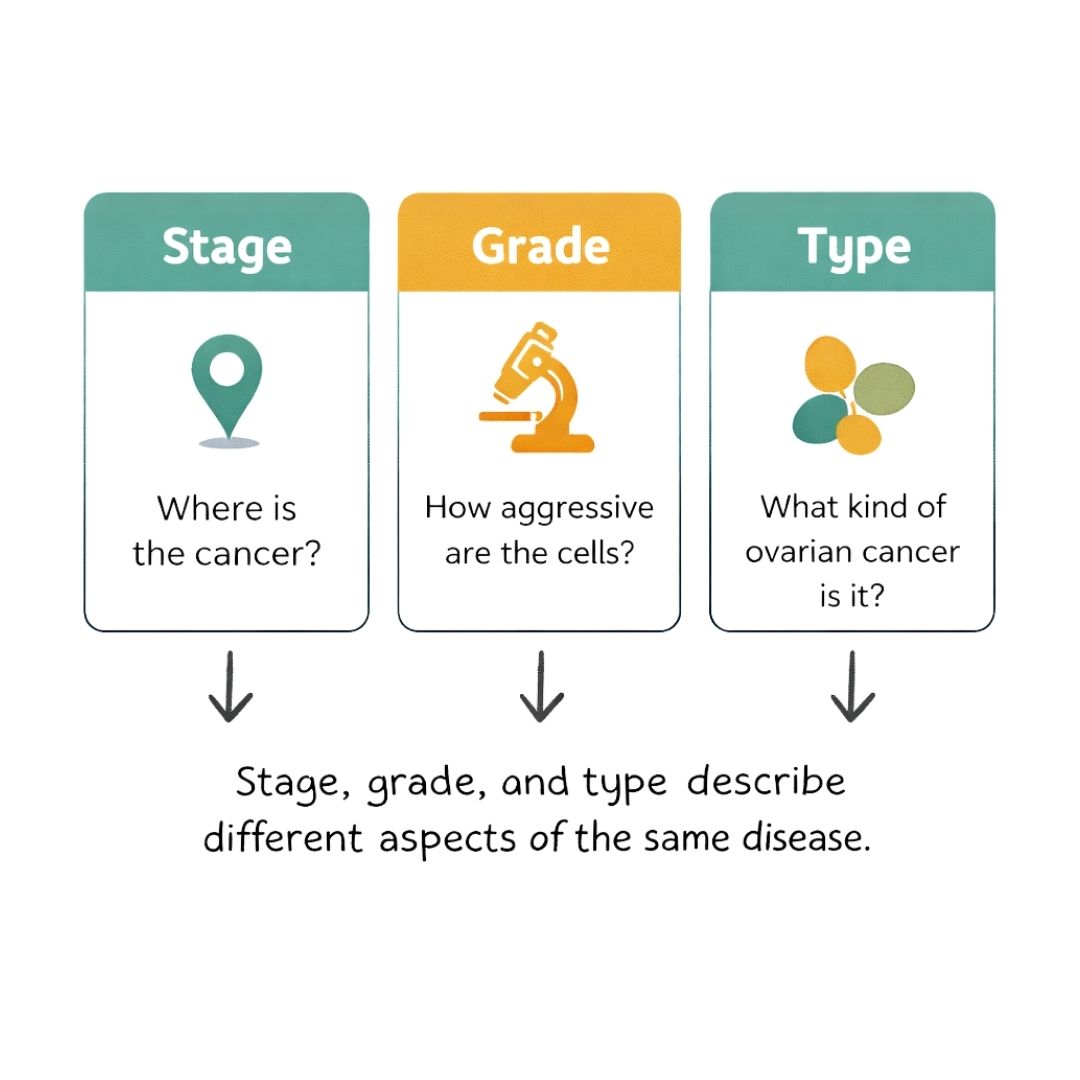
Knowing the stage of your ovarian cancer tells you where the disease is, but that's only part of the story. To build the most effective treatment plan, your medical team also needs to understand how the cancer is likely to behave. This is where tumour grade and type come into play.
These two factors add crucial layers of detail to your diagnosis. They help explain why two people with the same stage of cancer might follow very different treatment paths, and they empower you to have more informed conversations with your care team.
Put simply, the tumour grade describes what the cancer cells look like under a microscope. It’s a measure of how different they appear from normal, healthy ovarian cells, which gives us a strong clue as to how quickly the cancer might grow and spread.
Think of it like this:
Your tumour's grade is a key piece of the puzzle. A high-grade cancer at an early stage might be treated more aggressively than a low-grade cancer at the same stage because it carries a higher risk of coming back after initial treatment.
The final piece of your diagnosis is the tumour type, which tells doctors which kind of cell the cancer started from. Ovarian tumours are sorted into three main groups, and the detailed analysis required to identify them is a core part of laboratory medicine.
Epithelial Tumours
These are by far the most common, making up around 90% of all ovarian cancers. They start in the thin layer of tissue covering the outside of the ovaries (the epithelium). There are several subtypes, with the most frequent being serous, mucinous, and endometrioid carcinomas.
Germ Cell Tumours
Much rarer than epithelial tumours, these develop from the very cells that produce eggs (ova). They tend to affect younger women and teenagers and usually have a very good prognosis with the right treatment.
Stromal Tumours
This is another rare group. These cancers begin in the structural connective tissue cells that hold the ovary together and produce female hormones like oestrogen.
Understanding your specific combination of stage, grade, and type creates the complete diagnostic picture. This trio of "where," "how," and "what" allows your oncology team to design a treatment plan that gives you the best possible chance for a successful outcome.
When you’re first learning about the stages of ovarian cancer, it’s only natural for a lot of questions to pop into your head. A diagnosis is a complex thing to get your mind around, and it's completely normal to want clarity on what it all means for you and your future. This section aims to give you straightforward answers to some of the most immediate concerns people have.
The goal here is to help demystify the terminology and give you a solid foundation. Understanding these key points can make those conversations with your medical team feel less daunting and help you feel a bit more in control of your journey.
This is one of the first things many people ask, and it’s a great question. The stage you're given at diagnosis is a fixed point in time. It's essentially a snapshot of how far the cancer had spread when it was first discovered, and that classification doesn't change, even if the cancer grows or shrinks with treatment.
However, if the cancer comes back after you've finished treatment, this is called a recurrent cancer. While your original stage (say, Stage IIIC) will always remain on your medical record, the recurrence is treated as a new event. Your doctors will run new tests and scans to get a fresh picture of the situation and figure out the best way forward. So, while your initial stage isn't altered, this new assessment guides the next steps in your treatment.
Your stage at diagnosis is a permanent part of your medical history. If the cancer returns, it's called a 'recurrence.' Your care team will assess its current state to plan your new treatment, but the original stage classification remains the same.
It’s incredibly easy to mix up staging and grading, but they tell you two very different—and equally important—things about the cancer. You need both pieces of information to build a complete picture of your diagnosis.
Here’s a simple way to think about it:
Both staging and grading are critical for shaping your treatment plan. For instance, a low-grade cancer at an early stage might be treated very differently from a high-grade cancer at the very same stage.
For younger people especially, the impact of treatment on future fertility is a huge concern. Whether fertility-sparing surgery is an option is almost entirely dependent on the stage of the cancer.
In some very specific, early-stage cases, like a Stage IA diagnosis where the cancer is contained within a single ovary—it might be possible to perform surgery that removes only the affected ovary, leaving the uterus and the other healthy ovary intact. This could preserve the possibility of carrying a pregnancy in the future.
This is a deeply personal and complex decision that has to be balanced against the need to treat the cancer as effectively as possible. It calls for a detailed conversation with your gynaecological oncologist, who can walk you through the potential risks and benefits based on your exact diagnosis, tumour type, and grade.
Walking into your appointments with a few key questions can make a world of difference. When you're discussing the stages of ovarian cancer, your main goal should be to fully understand your personal diagnosis.
You might want to ask your care team:
Getting clear answers to these questions is the first step toward becoming an active partner in your own care.
We strongly advise you to talk with a health care professional about specific medical conditions and treatments.
The information on our site is meant to be helpful and educational but is not a substitute for medical advice.
Ovarian cancer what are the symptoms: Learn early signs, risk factors, and how to talk to your doctor.
Explore the prognosis for ovarian cancer in our guide. Learn about survival rates, influencing factors, and what to expect after diagnosis.
Despite PCOS And Cancer, Sarah Miraculously Conceived And Delivered A Healthy Baby, Showing Hope Thrives Against All Odds.
